*Corresponding Author:
Antoine Salloum,
Department of Dermatology, Saint George Hospital University Medical Center & University of Balamand, Beirut, Lebanon
Tel: +961 71143153
E-mail: antoine.g.salloum@gmail.com
Abstract
Background: Widespread asymptomatic papular eruption are common presentation to dermatology clinics. The differential diagnosis is wide and warrants a meticulous physical examination and complete history.
Objectives: Our aim is to differentiate clinically and on histopathology the diffuse eruption of asymptomatic papules that started on the abdomen.
Methods: We report a case of a 35-year-old female patient who presented for evaluation of a widespread asymptomatic papular eruption of about 10 years’ duration. Lesions started appearing on the abdomen, back and upper extremities, then, later on, the lower face and genitalia.
Conclusion: Syringoma is a benign sweat gland tumor formed by well-differentiated ductal elements of the eccrine glands. They are usually bilateral and symmetrically distributed, appearing mostly in crops as in our patient. They are flat topped, small skin colored or yellowish papules less than 3 mm in diameter. Many treatment modalities exist. Reassurance is best for generalized lesions.
Keywords
Diffuse papular eruption; Eruptive syringoma; Syringomas
Case Presentation
A 35-year-old female patient presented for evaluation of a wide- spread asymptomatic papular eruption of about 10 years’ duration. Lesions started appearing on the abdomen, back and upper extrem- ities, then, later on, the lower face and genitalia.
Physical exam showed multiple, 2-4 mm, skin colored to brownish papules, symmetrically distributed. Abdomen and back were severely affected (Figure1-2). Two to three lesions were noticed on the lower cheeks. Coalescing papules 6-8 mm were seen on genitalia leading to entire involvement of her vulvae. To note that her hands and distal parts of her lower extremities were spared. Her medical history was negative. Family history was vague with possible similar lesions re- ported on the abdomen of her grandmother. A biopsy specimen was obtained from one of the lesions.
What is your diagnosis?
- Urticaria Pigmentosa
- Eruptive Syringomas
- Disseminated papular granuloma annulare
- Eruptive Xanthomas
Diagnosis:
Eruptive Syringomas

Figure 1: Picture showing well demarcated, hyperpigmented, brownish papules with variable size on the back area.

Figure 2: Figure 2: Picture showing a closer look of the papules on the abdomen.
Microscopic Findings and Clinical Course
Histopathologic examination of one of the lesions revealed on H&E the presence of well-circumscribed, small comma-shaped tubular structures in the superficial dermis. The ducts were lined by two rows of flattened epithelial cells. The tubular structures were also surrounded by thickened collagen bundles. (Figure 3) Laboratory tests were done to rule out metabolic diseases which turned out to be normal. Unfortunately, the patient refused any medical or surgical treatment and she was lost to follow up.
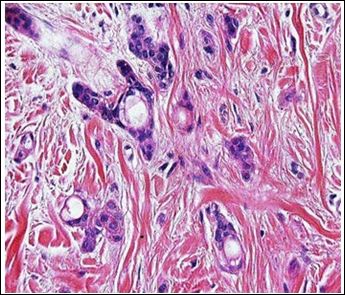
Figure 3: High Power H&E photomicrograph showing tadpole shaped tubules supported by a fibroblastic schirrous stroma.
Discussion
Syringoma is a benign sweat gland tumor formed by well-differentiated ductal elements of the eccrine glands [1].
Four variants have been recognized: a localized form, a form associated with Down’s syndrome, a familial form and a generalized form that encompasses multiple eruptive Syringomas. The development of syringomas, in crops and in large numbers is called eruptive Syringomas, and this type is a very rare variant of this kind of tumors [2]. The most common sites affected are the neck, axillae, anterior chest, upper abdomen, and periumbilical area [3]. A milium-like globoid structure overlies typical lesions of syringoma and this might be considered as a distinctive variant, reported by Zhong et al, which was the case in our patient.
Dermoscopically, fine pigment network with the typical rosette sign which is characterized by 4 white points arranged as a 4-leaf clover can be considered pathognomonic of this disease [4]. Syringomas affect 1% of the population and females are affected more often than males [2]. Lesions usually first appear at puberty; additional lesions develop later on [1].
They are usually bilateral and symmetrically distributed, appearing mostly in crops as in our patient. They are flat topped, small skin colored or yellowish papules less than 3 mm in diameter. Larger ones, which are the giant Syringomas, are rarely seen and in our patient, giant lesions are seen on the genitalia. They can be associated with pruritus which was absent in our case. They usually spare palms, soles and mucosal surfaces as our case demonstrated.
Eruptive syringomas might be associated with many diseases including Down’s syndrome, milium, elevation of carcinoembryonic antigen, diabetes, psychiatric disorders, Ehler Danlos syndrome, prurigo nodularis and sarcoidosis [5,6]. None of these was found in our patient.
On histopathology, lesions are located in the superficial dermis. They are composed of numerous small ducts in a sclerotic stroma. Some of the ducts have elongated tails of epithelial cells producing a characteristic comma-shaped or tadpole appearance.
In Urticaria Pigmentosa, the lesions are pruritic, exacerbated by friction (Darier Sign) [7]. In our patient, the lesions were asymptomatic and Darier sign was negative.
Disseminated papular granuloma annulare rarely involves genitalia and shows a lymphohistiocytic granuloma with connective tissue degeneration and mucin deposition unlike our patient [8].
Eruptive Xanthomas are reddish yellow papules arranged in crops on extensor surfaces, dorsum of the hands and buttocks and foamy macrophages are usually present on histopathology which were absent in our case [9].
For Syringomas, many modalities of treatment have been tried. For localized lesions; new techniques like microexcisions using Castroviejo scissors can minimize the risk of scarring [10], in addition to surgery, electrocautery and laser therapy which are usually used with different cosmetic results and possibility of scarring especially on the face. Reassurance is the best for generalized lesions.
References
- Soler-Carrillo J, Estrach T, Mascaro JM (2001) Eruptive syringo- ma: 27 new cases and review of the J Eur Acad Derma- tol Venereol 15: 242-246.
- Avhad G, Ghuge P, Jerajani HR (2015) Generalized eruptive sy- Indian J Dermatol 60: 214.
- Lau J, Haber RM (2013) Familial eruptive syringomas: case report and review of the J Cutan Med Surg 17: 84-88.
- Sakiyama M, Maeda M, Fujimoto N, Satoh T (2014) Eruptive sy- ringoma localized in intertriginous areas. J Dtsch Dermatol Ges 12: 72-73.
- Jamalipour M, Heidarpour M, Rajabi P (2009) Generalized erup- tive Indian J Dermatol 54: 65-67.
- Ozturk F, Ermertcan AT, Bilaç C, Temiz P (2010) A case report of postpubertal eruptive syringoma triggered with antiepileptic J Drugs Dermatol 9: 707-710.
- Middelkamp Hup MA, Heide R, Tank B, Mulder PG, Oranje AP (2002) Comparison of mastocytosis with onset in children and J Eur Acad Dermatol Venereol 16: 115-20.
- Thornsberry LA, English JC 3rd (2013) Etiology, diagnosis, and therapeutic management of granuloma annulare: An Am J Clin Dermatol 14: 279-290.
- Merola JF, Mengden SJ, Soldano A, Rosenman K (2008) Eruptive Dermatol Online J 14: 10.
- Todd PS, Gordon SC, Rovner RL, Tung R ( 2016) Eruptive Penile Syringomas in an Adolescent: Novel Approach with Serial Micro- excisions and Suture-Adhesive Repair. Pediatr Dermatol 33: 57-60.
Citation: Sakkal M, Salloum A, Debahy NES (2020) Widespread Asymptomatic Papular Eruption. J Clinic Exper Cosme Derma 3: 008.
Copyright: © 2020 Sakkal M, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
