*Corresponding Author:
Kafil Akhtar,
Department of Pathology, Jawaharlal Nehru Medical College, Aligarh Muslim University, Aligarh, Uttar Pradesh, India
Tel: 9568467727
E-mail: drkafilakhtar@gmail.com
Abstract
Krukenberg’s tumor is an uncommon metastatic tumor of the ovary, accounting for 1% to 2% of all ovarian tumors. Stomach is the most common primary site in most cases (70%). Pathologists have to be familiar with the diagnostic histopathologic features of the tumor and its principal differential diagnoses. Awareness of the diagnostic manifestations of the tumor leads to the correct diagnosis and prevents tumor misclassification, thus avoiding improper clinical management. We report a rare case of colorectal adenocarcinoma that presented as a unilateral Krukenberg’s tumor in a 45 year old female.
Keywords
Histopathology; Immunohistochemistry; Krukenberg’s Tumor; Unilateral
Introduction
Krukenberg’s tumor is an uncommon metastatic tumor of the ovary, first described in 1896 by Friedrich Krukenberg, a German gynaecologist and pathologist [1]. Stomach is the most common primary site in most cases of Krukenberg’s tumor (70%), followed by carcinomas of colon, appendix, and breast. Rare cases of Krukenberg’s tumor with primary carcinomas of the gallbladder, biliary tract, pancreas, small intestine, ampulla of Vater, cervix and urinary bladder have been reported [2].
Krukenberg’s tumor is uncommon, accounting for 1% to 2% of all ovarian tumors [3]. Pathologists have to be familiar with the diagnostic histopathologic features of the tumor and its principal differential diagnoses. Awareness of the diagnostic manifestations of the tumor leads to the correct diagnosis and prevents tumor misclassification, thus avoiding improper clinical management.
The prognosis of Krukenberg’s tumor is very poor. It is a known fact that signet ring cell adenocarcinomas of different organs tend to metastasize to the ovaries, with diffuse gastric adenocarcinoma being the most common [3,4]. The primary carcinoma in Krukenberg’s tumor is sometimes clinically occult and warrants a careful thorough examination of the gastrointestinal tract and other sites to detect the primary carcinoma [5].
Case Summary
A 45-year-old female presented with dull aching pain in the left lower abdomen with dyspeptic symptoms, anorexia, altered bowel habits and weight loss for the last 2 years. Ultrasound abdomen revealed a solid heterogeneous 10 cm × 7.8 cm left adnexal mass lesion with anechoic foci, separate from the uterus, urinary bladder and bowel loops with evidence of ascites. Ultrasonography of the abdomen also revealed an ill-defined mass lesion of 3 cm × 2.5 cm in the left iliac fossa. Complete blood count showed decreased haemoglobin levels and mild leucocytosis. Contrast enhanced CT abdomen showed an ill-defined heterogeneous poorly enhancing mass lesion of 8 cm × 6 cm size in the left adnexa with perilesional fat. Serum CA-125 was 143.8 U/ml.
Total abdominal hysterectomy with bilateral salpingo-oophorectomy was performed. The resected left ovary was asymmetrically enlarged, with a bosselated contour with solid yellow-white cut surface and smooth capsule (Figure 1).
Microscopically, sections showed 2 components: epithelial and stromal. The epithelial component was composed chiefly of mucin-laden signet ring cells with eccentric hyperchromatic nuclei and eosinophilic granular cytoplasm with mucin vacuoles (Figure 2 and 3).
With the suspicion of primary intestinal malignancy, lower GI endoscopy was performed, which revealed a 4 cm × 4 cm ulcerated lesion at the recto-sigmoid junction. Histopathology of biopsy specimen confirmed signet ring cell adenocarcinoma of mixed diffuse and intestinal type (Figure 4) with PAS positivity (Figure 5).
Immunohistochemistry was positive for pancytokeratin (Figure 6).

Figure 1: Grossly the resected left ovary was asymmetrically enlarged, with a bosselat- ed contour with solid yellow-white cut surface and smooth capsule.

Figure 2: Microscopically, sections showed epithelial component composed chiefly of mucin-laden signet ring cells with eccentric hyperchromatic nuclei and eosinophilic granular cytoplasm with mucin vacuoles. Hematoxylin and Eosin x 10X.
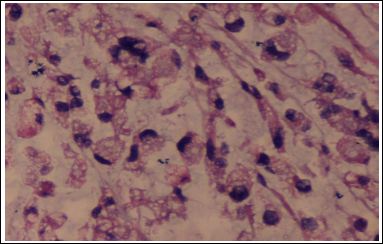
Figure 3: High power of Figure 2. Hematoxylin and Eosin x 40X.

Figure 4: Microscopically, sections showed scattered signet ring cells with eccentric hyperchromatic nuclei and eosinophilic granular cytoplasm admixed with atypical columnar cells. Hematoxylin and Eosin x 40X.

Figure 5: Microscopically tumor cells show PAS positivity. PAS x 40X.
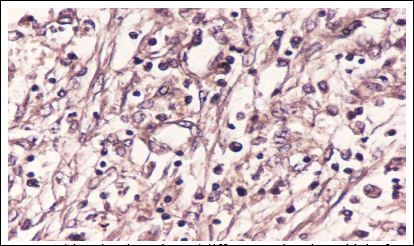
Figure 6: Immunohistochemistry showed diffuse cytoplasmic positivity for cytokeratin. IHC Cytokeratin x40X.
A diagnosis of metastatic colo-rectal adenocarcinoma with Krukenberg’s tumor was made and six 3-weekly cycles of palliative chemotherapy given with cisplatin and capecitabine. Our patient is doing well after 6 months of follow up.
Discussion
Krukenberg’s tumors tend to occur in the young females, with an average age of 45 years [6]. Common presenting symptoms are usually related to ovarian involvement, the most common of which are abdominal pain and distension (mainly because of the usually bilateral and often large ovarian masses). The remaining patients have nonspecific gastrointestinal symptoms or are asymptomatic [7,8]. Krukenberg’s tumor is also associated with virilization resulting from hormone production by the ovarian stroma [9]. Ascites is present in 50% of the cases and usually reveals malignant cells [8].
Stomach is the most common primary site of Krukenberg’s tumors, but other organs can serve as a primary site. The lymphatic system is the most likely route for metastasis.
The diagnosis of the primary carcinoma can be made either preoperatively, during the operation for the ovarian metastasis, or within a few months postoperatively [10]. Often, the primary tumor is too small to be detected. In such a situation, diagnosis of Krukenberg’s tumor warrants careful radiographic and endoscopic exploration of the digestive system in an attempt to detect the primary carcinoma [11]. Radiologically, Krukenberg’s tumors on abdominopelvic sonography and computed tomographic scans usually appear as bilateral solid to cystic ovarian masses [12].
The prognosis of a patient with Krukenberg’s tumor is extremely poor with average survival time between 3 and 10 months. Only 10% of patients survive more than two years after diagnosis [8]. Treatment of patients with Krukenberg tumor is still controversial. Some studies have demonstrated a prolonged survival after resection of both primary tumor and ovarian metastases.10Some other studies have suggested that metachronous ovarian metastases or unilateral ovarian metastases might correlate with good survival and ovarian metastasectomy may be beneficial [11].
Conclusions
Krukenberg’s tumor is a metastatic ovarian tumor that is histo- logically characterized by mucin-laden signet ring cells. Diagnosis of Krukenberg’s tumor with unknown primary warrants careful investi- gation of mainly the digestive tract and other potential sites. CA 125 levels can be used for screening for early detection of ovarian metasta- sis as well as for monitoring the course of disease.
References
- Krukenberg, Friedrich (1896) Uber das Fibrosarcoma ovarii muco- cellulare (Carcinomatoides). Arch F Gynak 50: 287-321.
- Miller RT, Sarikaya H, Jenison EL (1988) Adenocarcinoid tumor of appendix presenting as unilateral Krukenberg’s J Surg Oncol 37: 65-71.
- Lee KR, Young RH (2003) The distinction between primary and metastatic mucinous carcinomas of the ovary: gross and histologic findings in 50 cases. Am J Surg Pathol 27: 281-292.
- Baker PM, Oliva E (2005) Immunohistochemistry as a tool in the differential diagnosis of ovarian tumors: an update. Int J Gynecol Pathol 24: 39-55.
- Rosai J (2004) Rosai and Ackerman’s Surgical Vol 2. 9thed. St Louis, Mo: The CV Mosby Co; 1708-1718.
- Al-Agha OM, Nicastri AD (2006) An In-depth Look at Krukenberg’s Arch Pathol Lab Med 130: 1725-1730.
- Peng W, Hua RX, Jiang R (2013) Surgical treatment for patients with Krukenberg’s tumor of stomach origin: clinical outcome and prognostic factors analysis. PLoS One 8: e68227.
- Young RH (2006) From krukenberg to today: the ever present prob- lems posed by metastatic tumors in the ovary: part Historical perspective, general principles, mucinous tumors including the krukenberg’s tumor. Adv Anat Pathol 13: 205-227.
- Taylor AE, Nicolson VM, Cunningham D (1995) Ovarian metastases from primary gastrointestinal malignancies: the Royal Marsden Hospital experience and implications for adjuvant treatment. Br J Cancer 71: 92-96.
- Yook JH, Oh ST, Kim BS (2007) Clinical prognostic factors for ovar- ian metastasis in women with gastric Hepatogastroenterology 54: 955-959.
- Jun SY, Park JK (2011) Metachronous ovarian metastases following resection of the primary gastric J Gastric Cancer 11: 31-37.
- Das S, Sahu D, Wani M, Reddy PK (2014) A curious discourse of Krukenberg’s tumor: A case J Gastrointest Oncol 5: 117-120.
Citation: Akhtar K, Haiyat S, Anees A, Sherwani RK (2019) Unilateral Krukenberg’s Tumor-An Unusual Presentation. J Tissue Biol Cytol 3: 004.
Copyright: © 2019 Akhtar K, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
