*Corresponding Author:
Sokunbi Ganiyu,
Department of Physiotherapy, Bayero University, Kano, Nigeria
Tel: +234 08138468412
Email: ganiyusokunbi@gmail.com
Abstract
Background: Pain, fatigue and general reduction in physical activity have been common complications among kidney transplantation recipients. Medical treatments in the form of analgesics and narcotics currently used to relieve these symptoms are limited in their efficacy and not without side-effects. The facts that these medications has to be taking for a long time coupled with the fear of drug interactions has negative impact on patients compliance and made a lot of patients unwilling to take the option of chemotherapy.
Aims: This case study aimed to investigate the effects of motor control and moderate aerobic exercises, and acupuncture in the management of a post-transplant patient who was presented with severe back pain, fatigue and sexual dysfunction.
Methods: A 47-year-old man was presented in the physiotherapy department with complaint of back pain, fatigue and sexual dysfunction. The level of pain intensity and fatigue was assessed with Visual Analogue Scale and Brief Fatigue Inventory respectively. Sexual dysfunction was assessed with International Index of Erectile Function Questionnaire. Acupuncture, moderate aerobic and motor control exercises were carried out twice weekly for 12 weeks.
Results: Findings of this case study showed remarkable improvements with more than 80%; improvement in sexual function, reduction in the level of pain and fatigue after 12 weeks of treatment.
Conclusion: The outcome of this study has shown that motor control exercises, moderate aerobic exercises and acupuncture might be considered as complimentary treatment options where a post-transplant patient develop pain, fatigue and sexual dysfunction.
Keywords
Acupuncture; Exercise; Fatigue; Kidney transplant; Pain; Sexual-dysfunction
Introduction
Renal transplantation is the preferred treatment for patients with end-stage renal disease as it offers better quality of life and confers greater longevity than long-term dialysis. However, post-transplant kidney patients often experience various physical and psychological symptoms [1,2]. Pain, fatigue and general reduction in physical activity in allogeneic kidney transplantation recipients have always been of huge interest to rehabilitation specialists [3]. Pain is a common problem after kidney transplantation. Metabolic and cardiovascular burden of renal failure in addition to the impact of immunosuppressive treatment has made pain, fatigue and decline physical activity level common problems after kidney transplantation. Cyclosporine intake was identified for the first time as a novel reason for severe skeletal pain [4]. It has been reported that cyclosporine may induce bone marrow oedema leading to severe and disabling bone pain mainly located in the lower limbs [5]. Musculoskeletal pain after kidney transplantation could also be a manifestation of high-dose steroid therapy, steroid withdrawal, renal osteodystrophy or osteoporosis and neuropathy [5]. Displacements in the calcium phosphate vitamin D parathyroid hormone axis cause decalcification of the skeleton with the added risk of calcification of soft tissue [6]. Fatigue is a subjective feeling of tiredness that is influenced by circadian rhythms and can vary in unpleasantness, duration and intensity among post-transplant patient. Findings from a study support the assertion that moderate to severe feelings of fatigue exist commonly in post kidney transplant patients; these might probably be due to uraemia, reduced protein energy, anaemia and metabolic acidosis [4].
Because of the strong catabolic effects of kidney failure and post transplantation complications, a post-transplant patients need to exercise regularly to counter the decline in their aerobic fitness, muscle strength and endurance. Studies have shown that renal patients have the same relative ability to improve their aerobic fitness, muscle strength and endurance as healthy individuals of the same age regardless of whether they are at the pre uremic, dialysis or post-transplant stage [5,7]. However, there are other contributors to low exercise rates and fatigue in kidney transplant recipients. Patients may have attitudes or beliefs about exercise in relation to their health status and the possibility of injuring the graft may minimize their engagement in physical activity. Health care professionals managing kidney recipients may not provide sufficient counseling on the benefits of exercise for long-term health, perhaps because of other priorities within self-care management. Structural aspects of the health care system may undermine the ability of health care providers to systematically provide the appropriate guidance. Medical treatments in the form of analgesics and narcotics currently used to relieve the post-transplant pain are not without side-effects such as: dizziness, drowsiness, nausea, vomiting addiction and tolerance. The facts that these medications has to be taking for a long time coupled with the side effects has made a lot of patients unwilling to take the option of chemotherapy in the management of pain and other musculoskeletal complications. Pharmacological treatment may sometimes not have satisfactory effects [8].
Physiotherapy in the form of moderate aerobic exercises can be used to complement medical treatment for kidney transplant recipients. There is justification for recommending physiotherapy in the form of exercise to kidney transplant recipients. Sedentary behavior is a health risk factor that could exert its effect across a broad range of physiological indicators. Cardiovascular complication is one of the leading causes of death among kidney post-transplant patients and physical inactivity is a risk factor for cardiovascular conditions [7]. Exercise training can be beneficial in enhancing physical functioning after transplantation and substantially ameliorate the adverse sequelae of corticosteroids and deconditioning from years of dialysis therapy [7]. Moreover, there are no documented adverse consequences attributed to physical activity in kidney transplant recipients. Acupuncture is widely used to treat common symptoms such as pain, fatigue and depressive mood in patients with chronic conditions.
Phosphodiesterase type 5(PDE-5) inhibitors (e.g., sildenafil, Viagra; tadalafil, Cialis; vardenafil, Levitra) are among the drugs of choice for Erectile Dysfunction (ED). PDE-5 inhibitors function by relaxing smooth muscle thereby allowing the penis to fill with blood. PDE-5 inhibitors work in approximately 7 of 10 men but may lose their effectiveness if taken over a long period of time [8]. The beneficial effects of PDE-5 inhibitors diminished over time to thee point whereby patients no longer able to maintain an erection despite continuous use of these medications. Manual Acupuncture carried out at BL-33, Zhongliao acupuncture point has been reported to have positive effects as improved confidence and hardness of the erection and maintenance of the erection during sex to completion of sexual inter course [9]. It could also be that the combined analgesic and neuroendocrine effects of exercise and acupuncture will make these treatment modalities useful adjuncts in combating pain, fatigue and reduced physical activity level in kidney post-transplant patients [10]. Thus, this case study aimed to investigate the effects of motor control and moderate aerobic exercises and acupuncture in the management of a post-transplant patient who was presented with sever back pain, fatigue and sexual dysfunction.
Case Presentation
A 47-year-old man was presented in the physiotherapy department in August 2014. He is a known hypertensive and chronic kidney disease patient. Subsequently, he had renal allograft failure in the year 2000 leading to dialysis for 10 years. Three years prior to referral to physiotherapy, he received another successful renal transplant but was presented in the physiotherapy clinic with complaints of back pain, easy fatigability and erectile dysfunction. Patients reported that his pain worsens in an upright standing, prolonged sitting positions and during movement Patient also reported recurrent dyspnea with mild to moderate exertion and multiple episodes of paroxysmal nocturnal dyspnea over the past 6 months. He experienced Erectile Dysfunction (ED) after initiation of dialysis treatment which was reported to have gotten progressively worse. Patient was placed on 25mg Sildenafil which was initially successful in controlling ED, however, its therapeutic effects waned after 2 weeks of usage. A suggestion was given to increase l the dosage of Sildenafil to 50mg but patients expressed reservation because of the possible side effects and concerns for potential drug interactions. Patient reported taken 500mg of acetaminophen for pain twice daily prior to the commencement of acupuncture and therapeutic exercises used in this study.
Physical Examination and Pre-intervention Assessment
On examination, patient has mesomorphic body somatotype. He walks slowly with an antalgic gait, reduced lumbosacral lordosis, symmetrical pelvic and normal lower extremities alignments. Posterioanterior (PA) thrust elicited pain at first lumbar (L1) down to the fifth lumbar (L5) spinal segments. Active spinal Range of Movements (ROM) was carried out using Schober’s method [11]. It showed that spinal ROM was limited by more than 50% in all directions. Positive prone instability test was carried out by asking the patient to lie on the plinth with the trunk, head and arms while the feet are on the floor. A Posterioanterior pressure was applied to the spinous processes of the lumbar spine. Painful provocation was recorded at L1 down to L5. The patient was then asked to raise one leg up off of the floor and PA pressure is again applied to the spine. A reduction in pain while the leg is raised is (a positive test) was observed at L1 down to L5. Straight Leg Raise (SLR) was 100 degrees on both sides: SLR test was carried out with the patient in supine lying position, it did not show any sign of lumbosacral nerve root compression. The International Index of Erectile Function (IIEF) Questionnaire, a validated instrument was used to assess the severity of ED [12]. The IIEF-5 score is the sum of the ordinal responses to the 5 items with a total possible score of 25. The lower score the more severe the sexual dysfunction. A score of 22-25 implies no erectile dysfunction while a score of 5-7 depicts severe erectile dysfunction [12]. Brief Fatigue Inventory (BFI) was used to assess the severity of fatigue. BFI measures the severity of fatigue and is impact on daily activities. BFI has a Cronbach alpha reliability which ranges from 0.82 to 0.97 [13]. Visual Analogue Scale (VAS), a validated instrument, was used to assess his level of pain [14]. The blood pressure measured 148/80, pulse was 72 beats per minute, respiratory rate was 12 breaths per minute were recorded on the first visit. The lumbar spine plain X-ray did not show any features of bones and joint pathology. Assessments were carried out on weekly basis prior to the commencement of treatment in the beginning of every week.
Clinical Reasoning
Lumbar spine X-ray did not show any features of bone and joint pathology, findings from the subjective and physical examination suggest that this particular patient lack spinal segmental control as indicated by positive prone stability test which could be responsible or partly responsible for the complaint of back pain. Thus, there are possibilities that this patient will benefit from the use of spinal segmental motor control exercise like core stability exercise to relieve the pain and the use of moderate aerobic exercise to increase the aerobic level and reduce the fatigue level. Erectile dysfunctional problem reported by this patient could be due to a reduction and/or dysfunction in the serum level of sexual hormones or perhaps more complex neurohormonal disorders or perhaps due to other mechanisms not yet well investigated. Besides, the central and the peripheral mechanisms of acupuncture induced analgesia which might be useful to effect pain reduction. It is also possible that the reflex action induced by acupuncture stimulation leading efferent discharge of sympathetic nerve innervating internal organs (somato-sympathetic reflex), a kind of neuroendocrine-autonomic responses that is predominantly mediated by Hypothalamic Pituitary-adrenal axis (HPA) might be useful to address the problem of ED. A combination of acupuncture and therapeutic exercises was used in this present study because studies have shown that, in the short term, acupuncture has a positive effect on relief from chronic low back pain, but when compared to conventional or alternative therapies, it was found not to be any more effective in reducing pain. However, when applied in conjunction with conventional therapies such as therapeutic exercises, greater improvement might be seen.
Interventions
Motor control exercise
Motor control exercise was carried out. It is made up of demonstrations and instructions on how to activate the core muscles of spinal stabilization, 5-minutes warm up with stretching exercises to the upper and lower back muscles, 20 minutes of main exercises in supine lying, prone kneeling, sitting and standing positions and 5 minutes of cool down stretching exercises [10]. The exercise was carried out twice a week for twelve weeks.
Moderate aerobic exercises
Aerobic training was carried out on a stationary bicycle at an intensity of 12-16 out of 20 at the Rate of Perceived Exertion (RPE) of Borg scale so that intensity involved 65-85% of an individual’s maximal heart rate capacity, a level at which cardiovascular health can be obtained. The Borg scale is a simple method of RPE and can be to gauge level of intensity during exercise performance. There are a number of RPE scales but the most common are the 15-point scale (6-20). The exercise program consisted of a 5-min warm up, a 20-min cycling, and a 5-min cool down period [14]. The exercise was carried out twice a week for twelve weeks.
Manual acupuncture needle stimulation
The patient received manual acupuncture treatment administered by a certified Acupuncturist with more than 9 years of clinical experience. The treatment was carried out twice a week for twelve weeks. Acupuncture was given at the following acupuncture points; Pangguangshu BL-28 point (1.5cun off midline along the posterior sacral second foramen), Shenshu BL-23 point (1.5cun lateral to the lower edge of spinous contour of the second lumbar vertebra), Yinlingquan SP-9 (point on the medial of the shin or trough induced by the angle between internal tibia condyle and posterior tibia surface). Disposable 0.25 mm×30 mm or 40 mm acupuncture needles were used. The needles were inserted to a depth of 0.2 to 10 mm, according to the location of points, and remained in place for 30 min. Manipulation for de-qi (eliciting an aching and dull sensation) was repeated every 5minutes intervals. These three acupuncture points were chosen for their location on the spleen and bladder meridian path. The selected acupuncture points used in this study have been reported to be effective in balancing the energy flow and revitalize the reproductive organs to promote better functioning [15,16].
Results
Patient reported a score of 8cm out of 10cm for pain intensity and 90 of 100 for the level of fatigue at the beginning of the treatment. Assessments of pain intensity and level of fatigue were carried out on weekly basis and the results are presented in Figures 1&2 respectively. It is remarkable to note a sharp kink in both graphs at 6 weeks of treatment, the point at which at least 50% reduction in pain intensity and fatigue level were achieved. Subsequently more than 90% reduction in both pain and fatigue level were achieved at 12 weeks. Patients reported complete cessation from any form of medications due to improvement with pain reduction after six weeks of treatment.
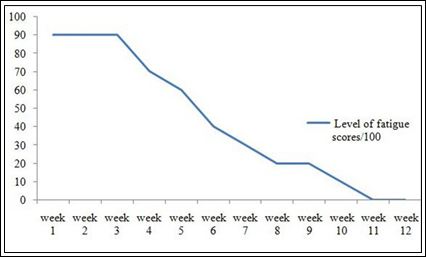
Figure 1: Changes in pain intensity during treatment.
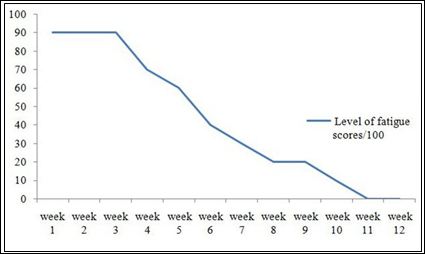
Figure 2: Changes in the level of fatigue during treatment.
The Erectile function also improves progressively during the treatment with about 40% and 88% increase after 6 weeks and 12weeks of treatment respectively (Figure 3).
Discussion
Musculoskeletal pain and fatigue are common problems caused by metabolic and cardiovascular burdens of renal failure and post kidney transplant complications. However, it is not yet well clarified, the degree to which each of the metabolic and cardiovascular burdens contribute to the problem of pain, fatigue and reduced level of physical activity among post-transplant kidney patients. Musculoskeletal disorders in this group of patient could also be linked to some other aetiological factors such as; Calcineurin Inhibitor-induced Pain Syndrome (CIPS), polyneuropathy, osteoporosis, hyperparathyroidism, reflex sympathetic dystrophy or avascular bone necrosis [3].
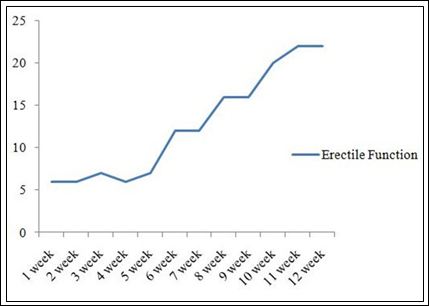
Figure 3: Changes in erectile function during Intervention.
Findings from this case study have demonstrated significant reduction in the level of pain intensity and fatigue following treatment with acupuncture, motor control and moderate aerobic exercises. The positive effects of acupuncture on postoperative pain in renal patients has been reported by Tabassi et al., [17] who carried out a study on the effects of acupuncture on pain among post nephrectomy patients. Findings from their study showed that pain severity was significantly lower in the acupuncture group than in the sham group and the mean opioid demand in the sham group was significantly more than that in the acupuncture group. Studies have shown that in the short term, acupuncture has positive effects on relief from pain but when compared with conventional or alternative therapy, it was not found to be more effective but when combined with other therapy greater improvement may be seen [10]. The present case study has shown that remarkable pain relief may occur when acupuncture is combined with core stability and moderate aerobic exercises.
Stabilisation exercises induced analgesic effects has been linked to improved pattern of activation and onset of activity in the core muscles of spinal stabilisation especially the transversus abdominis and the multifidus and reduce which primarily act like a corset for the spine to maintain segmental spinal stability to reduce pain and pain recurrence in patients with chronic spinal pain [10]. More so, promotion of moderate aerobic exercises in a kidney transplant patients have been opined to have the benefit such as; stimulation of the endothelium of blood vessels to improves circulation, lower blood pressure and heart rate at rest and during exercise as well as enhancing metabolic processes of oxidation of glucose and fatty acids, and lowering of cholesterol [3,17]. Other benefits of moderate aerobic exercises include regulation of secretion systemic hormones, reduction of oxidative stress influencing secretion of cytokines, leading to reduction in the fatigue level and improvement in the patient quality of life [3,18,19].
The numerous beneficial effects of exercises leading to improvement in the quality of life a post-transplant patient seems to generate a question of why many post-transplant patients are unwilling and reluctant in engaging in exercises after their transplant. It could be that these patients have got the fear of injuring the transplanted graft, and/or on the transplant professionals’ silence about the benefits of exercise. The cause can sometimes be the protective attitude of the family members and friends. Moreover, patients of diverse ethnic and cultural backgrounds may place differential values on exercise and self-care or this lack of importance given to physical training can be the consequence of the absence of structural support.
Findings from this study also showed positive results in the form of increasing sexual function of the patient. Among post-transplant kidney patient erectile dysfunction is a commonly observed sexual problem whose etiology could be multifactorial arising from a complex neuroendocrine and metabolic changes [20]. Several treatment options such as chemotherapy for erectile dysfunction exist, however reports on its wide use among post-transplant patients seems to be lacking and there are concerns about the patients compliance [20]. There is dearth of evidence, based on rigorous research on the efficacy of acupuncture on erectile dysfunction among kidney transplant patient. A systematic review on the effects of acupuncture on erectile dysfunction showed beneficial effects of acupuncture compared with sham acupuncture in terms of response rate [20]. This review concluded that it may be valuable to investigate acupuncture as a non-pharmacological treatment options in a field where the evidence of conventional therapies is also limited. It is also possible that the reflex action induced by acupuncture stimulation leading to efferent discharge of sympathetic nerve innervating internal organs could be partly responsible for the recovery from erectile dysfunction of the patient in this case study.
Conclusion
The outcome of this study has shown that motor control exercises, moderate aerobic exercises and acupuncture might be considered as a complimentary treatment option where a post-transplant patient develop pain, fatigue and sexual dysfunction. However, this present study is limited because as a single case study, so the results cannot be generalized. A larger randomized controlled trial with a longterm follow up is needed to make the findings more generalizable.
References
- Jablonski A (2007) The multidimensional characteristics of symptoms reported by patients on Nephrol Nurs J 34: 29-37.
- Murtagh FE, Addington-Hall J, Higginson IJ (2007) The prevalence of symptoms in end-stage renal disease: a systematic review. Adv Chronic Kidney Dis 14: 82-99.
- Chang WK, Hung KY, Huang JW, Wu KD, Tsai TJ (2001) Chronic fatigue in long-term peritoneal dialysis Am J Nephrol 21: 479-485.
- Piper BF, Dibble SL, Dodd MJ, Weiss MC, Slaughter RE, et al. (1998) The revised Piper Fatigue Scale: psychometric evaluation in women with breast Oncol Nurs Forum 25: 677 -684.
- Grotz WH, Breitenfeldt MK, Braune SW, Allmann KH, Krause TM, et al. (2001) Calcineurin-inhibitor induced pain syndrome (CIPS): a severe disabling complication after organ Transpl Int 14: 16-23.
- Guarnieri G, Toigo G, Situlin R, Faccini L, Coli U, et (1983) Muscle biopsy studies in chronically uremic patients: evidence for malnutrition. Kidney Int Suppl 24: 187-193.
- Boyce ML, Robergs RA, Avasthi PS, Roldan C, Foster A, et al. (1997) Exercise training by individuals with predialysis renal failure: Cardiorespiratory endurance, hypertension, and renal Am J Kidney Dis 30: 180-192.
- Sugawara Y, Akechi T, Shima Y, Okuyama T, Akizuki N, et al. (2002) Efficacy of methylphenidate for fatigue in advanced cancer patients: A preliminary Palliative Medicine 16: 261-263.
- Taniguchi H, Imai K, Taniguch S, Kitakoji H (2014) Acupuncture in the Treatment of Erectile Dysfunction among a Diabetic Population of Sildenafil Citrate Non-Respnder. Japanese Acupuncture and Moxibustion 10: 14-17.
- Sokunbi OG, Kachalla FG (2015) Effects of Acupuncture, Core-stability Exercises, and Treadmill Walking Exercises in Treating a Patient with Postsurgical Lumbar Disc Herniation: A Clinical Case Report. J Acupunct Meridian Stud 8: 48-52.
- Viitanen JV, Kautiainen H, Suni J, Kokko ML, Lehtinen K (1995) The relative value of spinal and thoracic mobility measurements in ankylosing Scand J Rheumatol 24: 94-97.
- AHRQ Publication (2009) Diagnosis and Treatment of Erectile Dysfunction. Rockville, Maryland, USA.
- Lin CC, Chang AP, Chen ML, Cleeland CS, Mendoza TR, et al. (2006) Validation of the Taiwanese Version of the Brief Fatigue J Pain Symptom Manage 32: 52-59.
- Jensen MP, Karoly P, Braver S (1986) The measurement of clinical pain intensity: a comparison of six methods. Pain 27: 117-126.
- Lee MS, Shin BC, Ernst E (2009) Acupuncture for treating erectile dysfunction: a systematic BJU Int 104: 366-370.
- Johansen KL (2005) Exercise and chronic kidney disease: current recom Sports Med 35: 485-499.
- Tabassi KT, Amini P, Razavizadeh RT, Mohammadi S (2015) Effects of acupuncture on pain score following open kidney surgery Pars. Journal of Medical Sciences 12: 29-37.
- Romano G, Simonella R, Falleti E, Bortolotti N, Deiuri E, et al. (2010) Physical training effects in renal transplant Clin Transplant 24: 510-514.
- Painter PL, Hector L, Ray K, Lynes L, Paul SM, et al. (2003) Effects of exercise training on coronary heart disease risk factors in renal transplant recipi Am J Kidney Dis 42: 362-369.
- YeniçerioGlu Y, Kefi A, Aslan G, Cavdar C, Esen AA, et al. (2002) Efficacy and safety of sildenafil for treating erectile dysfunction in patients on BJU Int 90: 442-445.
Citation: Ganiyu S (2018) Therapeutic Exercises and Acupuncture in the Management of Back Pain and Erectile Dysfunction in a Kidney Post Transplant Patient- A Case Study. J Acupun Tradit Med 2: 003.
Copyright: © 2017 Ganiyu S. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.