*Corresponding Author:
Tantri AR,
Department of Anesthesiology and Intensive Care, Faculty of Medicine, Universitas Indonesia, Jl. Salemba Raya no.6, Central Jakarta 10430, Jakarta, Indonesia
Tel: +628161832487
Email: aidatantri@yahoo.com
Abstract
Background: Prediction of skin-epidural distance on paediatric patient is necessary to avoid paediatric epidural anesthesia complications. Bosenberg prediction formula of 1 mm/kg of body weight was widely used in Caucasian paediatric patients. However, there are anatomical variations between Caucasians and Asians, which leads us questioning the accuracy of Bosenberg formula of 1 mm/kg in predicting the distance between the skin and epidural space in paediatric Malayan patients, and which factors contribute in determining epidural space depth.
Methods: This was a retrospective cross-sectional study, subjects included were 53 Malayan paediatric patients who had underwent epidural anesthesia in Cipto Mangunkusumo Hospital in January 2011 July 2015. After approval from Universitas Indonesia Ethics Committee, age, weight, height and actual loss of resistance distance from skin data were collected and analysed. SPSS 22 was used to perform statistical calculation on this set of data. Accuracy of Bosenberg formula was analysed using Bland-Altman test by comparing the actual Loss of Resistance (LOR) distance with predicted LOR from Bosenberg formula. Linear regression analysis was used to identify variables that had predictive value to skin-epidural distance.
Result: Limit of agreement between the actual Loss of Resistance (LOR) distance with predicted LOR from Bosenberg formula were -4.41 to 3.15, which was significantly larger than the expected limit of agreement (-1.25 to 1.25). There was a strong corelation between age, weight and height to skin-epidural distance. Patient’s weight had the strongest power to predict skin-epidural distance. R2 value for weight, height and age were 92.7%, 75.9% and 57% respectively.
Conclusion: The Bosenberg prediction formula of 1 mm/kg of body weight is not accurate to predict skin-epidural distance in Malayan paediatric population. There is a strong relationship between patient’s age, height, and weight to skin-epidural distance in Malayan paediatric patients.
Keywords
Age; Height; Loss Of Resistance (LOR); Paediatrics; Skin-epidural distance; Weight
Introduction
Dural puncture as a complication of epidural anesthesia in paediatric patients can be reduced by improving the anesthesiologists’ ability to predict the skin-epidural distance, thus improving the safety of epidural anesthesia [1-3]. Anesthesiologists can insert the epidural needle more carefully when it has a close proximity to the prediction value of skin-epidural distance.
The skin-epidural distance in L2-L3 is around 10 mm in neonates [4]. This depth increases linearly according to the age. Body weight and height also contribute in determining the skin-epidural space distance [4,5]. There are several formulas to determine Skin to Epidural space Depth (SED), one of them is Bosenberg formula who has two alternatives, SED (mm) = 0.8 mm x weight (kg) + 3.93 mm, and the simplified formula SED (mm) =1 mm x kg body weight to improve safety and success rate in the epidural anesthesia procedure [5]. The Bosenberg formula is the most widely used formula to predict skin-epidural distance in paediatrics patients, especially in Caucasians. Different populations and races present different anatomy of vertebrae. Moreover, Uemura also has a formula for paediatrics in Japan, SED (mm) = 0.8mm x weight (kg) + 8 mm [6].
Since anatomical difference can reduce the accuracy of Bosenberg formula, this study aimed to find out whether the Bosenberg formula is accurate in predicting skin-epidural distance in Malayan paediatric patients. This study also aimed to find out the correlation between patient’s age, weight, and height to the actual skin-epidural distance, and to found the formula to predict skin-epidural distance in Malayan paediatric patients.
Methods
This was a retrospective cross sectional study in Cipto Mangunkusumo Hospital, Jakarta, Indonesia which included Indonesian Malayan paediatric patients ASA I-III in the age range of 6 months to 10 years old who had elective surgical operations in January 2011- July 2015 with lumbal epidural anesthesia insertion at L4- L5 with needle angle 0-300 (in accordance with Cipto Mangunkusumo hospital’s Standard Operating Procedure). Patients with vertebrae malformations, underweight or obese based on <5% and >95% percentiles, were excluded. Forty seven subjects were needed for this study based on descriptive research with numeric variables sample formula and linear regression sample formula calculation. After ethical clearance from Universitas Indonesia Ethics Committee, patients’ age, weight, height, and predicted skin-epidural distance with Bosenberg formula data were collected. The actual skin-epidural distance recorded was the depth of the needle measured in mm when reached the epidural space with loss of resistance technique using syringe prefilled with normal saline and confirmed then with smooth epidural catheter insertion.
Data analysis was done using SPSS 22. Bland Altman test was done to test the accuracy between predicted skin to epidural distance by Bosenberg formula and the actual Loss of Resistance (LOR). The Bosenberg formula that was compared to in this study was the simplified formula of SED (mm) = 1 mm x weight (kg). The limit of agreement value was calculated using this formula:
Limit of agreement = mean difference ± 1.96 x standard deviation
Linear regression analysis was done to find out which of the three variables has the strongest correlation towards LOR.
Result
Fifty three patients were included in this study, from January 2011 - July 2015. Subject characteristics were presented in Table 1. The number for male patients is 52.8% which was almost the same number with female patients, 47.2%. The median for subjects was 63 months, with 6 months being the youngest and 116 months being the oldest. Mean for body weight was 16.5 kg, with 6.8 kg as the lightest weight and 35 kg as the heaviest weight. Mean for height was 101.5 cm with range 65 cm to 140 cm. In this study, the median LOR was 15 mm with LOR ranges from 7 mm to 40 mm. There were no complications of epidural anesthesia found in this study (dural puncture, infection and hematoma).
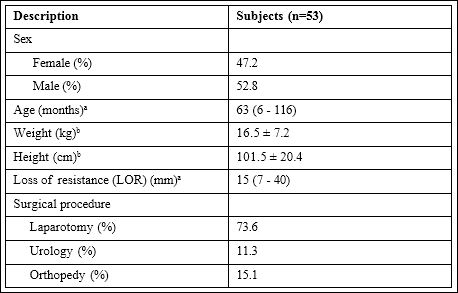
Table 1: Subjects’ Characteristics
aPresented in median (minimum-maximum)
bPresented in mean ± standard deviation
Mean actual skin - LOR distance in this study was 17.151 mm. This value is larger than mean predicted Bosenberg skin- epidural distance which was 16.519 mm (Table 2). The mean difference between the actual and Bosenberg LOR was -0.632.

Table 2: The mean value of LOR.
Limit of agreement between predicted Bosenberg skin-epidural distance and actual skin - LOR distance were -4.41 mm to 3.15 mm (Figure 1). The predicted Bosenberg skin-epidural distance could have difference as much as 3.15 mm more or 4.41 mm less than the actual skin - LOR distance.

Figure 1: Bland-Altman test result of the actual LOR towards Bosenberg LOR. Limit of agreement -4.41 to 3.15, mean difference -0.632 (CI 95% -1.164 to -0.100).
Spearman test result showed a positive correlation in the Table 3. The strongest correlation belongs to age (R = 0.09), followed by weight (R = 0.966) and height (R = 0.906). Data synthesis of the three variables showed p < 0.001 with p-value significance of 0.05.

Table 3: Correlation between Age, Weight, and Height to the Actual LOR.
*Spearman test, p-value significance 0.05
There were multicollinearity correlations between each variables to the actual LOR, thus analysis can only be done using linear regression, which resulted in three equations to predict the skin- LOR distance (Table 4).

Table 4: Linear Regression Equation to Determine Skin-Epidural Space (LOR) towards Each Variable.
Weight had the strongest correlation with skin LOR distance (R2 = 92.7%), compared to age (R2 = 57%) and height (R2 = 75.9%). Figure 2 showed the scattered diagram of the actual skin - LOR distance towards predicted standardized weight value obtained from the linear regression equation.
Discussion
Subjects in this research are paediatrics in 6 months to 10 years age. This age range was chosen due to similar age characteristics in Bosenberg’s study. In Bosenberg’s study, the mean age of the subjects was 54 months and the mean weight was 15.7 kg, while in this study the mean age was 59.7 months and the mean weight was 16.5 kg. Based on these data, the subjects’ characteristic in this study does not differ much from Bosenberg’s. The mean LOR of this study was 17.1 mm while mean LOR in the Bosenberg’s study was not mentioned [1].
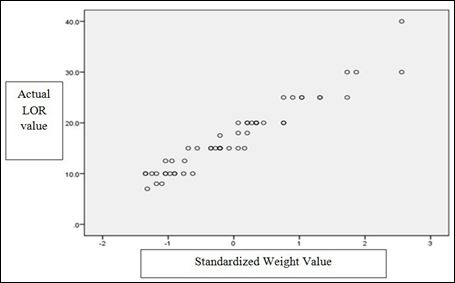
Figure 2: suggests a positive linearity between the predicted LOR value based on the weight and the actual LOR. Thus, the linear regression assumption of this study was fulfilled.
Scattered diagram of the Actual LOR towards Standardized Weight Value
Range of difference allowed between predicted and actual value had been determined as 2.5 mm (-1.25 to 1.25 mm) prior to this study. This value was determined based on the accuracy of epidural needle depth measurement which is 2.5 mm. The limit of agreement obtained was -4.41 mm and 3.15 mm, which were much larger than the difference allowed. Bosenberg’s formula did not accord with the actual skin-LOR distance in Malayan paediatric patients’ age 6 months to 10 years.
The inaccuracy of the Bosenberg’s formula in predicting the skin-epidural distance in this study can be due to several factors, such as the differences of subcutaneous fat thickness, differences of vertebrae anatomy between Malayans and Caucasians, and the difference of the measurement angle while doing the epidural anesthesia.
Gurrici et al., [7] stated that Malayans in Indonesia had larger body fat composition than Caucasians with the same Body Mass Index (BMI). Wang et al., [8] stated that Asians has smaller BMI and larger percentage of body fat than Caucasians in the same age population and sex. Based on those studies, racial difference could cause a difference in the body fat composition, including subcutaneous fat distribution between Asians and Caucasians although both are in the same age and sex groups. The presence of thicker subcutaneous fat could contribute to bigger skin-epidural distance.
Tan et al., [9] stated that Asians had bigger corpus vertebrae than Caucasians, which should cause smaller skin-epidural distance due to the relative dorsal propulsion of the epidural space. Malayan had more subcutaneous fat than Caucasians’ which causes larger skin-epidural distance despite of the bigger corpus vertebrae. Smaller skin-epidural distance in Asians compared to Caucasians was also reported in Uemura’s study about paediatrics in Japan. Uemura [6] suspected the difference in the skin-epidural distance is also caused by the patients’ height. Japanese patients were shorter than Caucasians despite of the same body weight, which causes addition in the subcutaneous fat in the Japanese and resulted in the larger skin-epidural distance [6,10].
Epidural anesthesia in Uemura’s study was done at lumbal level L3- L4, while in this study the puncture level was at L3-L4 to avoid dural puncture in paediatrics.
Moreover, the difference in the skin-epidural distance can be due to the different technique of epidural needle insertion. Bosenberg stat ed that the skin-epidural distance can increase up to 1.5 mm in the 30o angle [11]. In this study, we did not record the exact needle insertion angle for every puncture. Further prospective study recording certain needle insertion angle data is needed to assess the accuracy of the Bosenberg’s formula in paediatric Malayan patients aged 6 months to 10 years old.
In the bivariate analysis there were significant correlations be tween age, body weight and height as variables. This study stated that body weight had the strongest correlation as a factor that contributes to the skin-epidural distance in paediatric Malayan patients aged 6 months to 10 years old. Similar findings were stated by Bosenberg, Hasan, Uemura, and Franklin [1,5,9-11]. This similarity might be due to the increased subcutaneous fat which causes increased skin-epidur al distance.
The equation to predict the skin-epidural distance obtained from linear regression analysis based on the age and body weight had weaker correlations than the body weight. The accretion of the age causes an increase in body weight and height. In the paediatrics, the height will continue to increase and stop when the person is full-grown [12].
The age accretion will cause anatomical changes in the vertebrae, which affects the skin-epidural distance. As the age gets older, the skin-epidural distance gets bigger. The addition of the distance is not caused by the addition of age only, but also weight and height growth as well.
Wu et al., stated that height had a negative correlation towards subcutaneous fat in posterior part of the body [13] Height growth without weight increase causes lesser skin-epidural distance due to less subcutaneous fat. Subjects in this study were patients with height growth accompanied with weight addition, thus causing deeper skin-epidural distance, which is also shown with linear regression equation in this paper. To conclude, the increasing age, weight and height will cause deeper skin-epidural distance.
The prediction value of the skin-epidural distance obtained from the linear regression equation based on age, weight and height had a good correlation with the actual skin-epidural distance in paediatric Malayan patients. The strongest correlation value belongs to weight (R2= 92.7%). Thus the equation to predict the skin-epidural distance obtained from linear regression analysis based on the weight was ac- curate to use in Malayan paediatric patients:
Skin-epidural distance (LOR) = 1.912 + (0.922 x kgBW) mm
Limitation of the study include the retrospective method that this study used (the data was obtained from medical records) and the measurement bias that could arise from different operators since there was no standardization of operators’ skill in doing epidural anesthesia eventhough all operators were in the same educational stage. The dif- ference in measuring needle distance could affect the prediction val- ues result of skin-epidural distance in the Malayan paediatric patients.
Conclusion
The Bosenberg’s formula was not accurate in predicting the skin-epidural distance in Malayan paediatric patients aged 6 months to 10 years old. Age, weight, and height had significant correlations with the skin-epidural distance in the patients. The formula to predict skin-epidural distance obtained by the linear regression analysis based on weight was accurate to use in the Malayan paediatric patients aged 6 months to 10 years old in Cipto Mangunkusumo Hospital.
Disclosures
- Ethical approval: Approval from Faculty of Medicine Universitas Indonesia Ethics Committee had been obtained prior to the
- Funding: This research was carried out without
- Conflicts of interest: No conflicts of interest
References
- Bosenberg A (2011) Regional anesthesia central neuraxial blocks. Bissonnette B (eds.). In: Paediatric Anesthesia Basic Principles-State of the Art-Fu- People’s Medical Publishing House, USA, Pg no: 806-812.
- Dalal P, Davies CW (2005) Skin-epidural distance in paediatric patients: an Anaesthetic Department, Guy’s Hospital London. (Cited March 18th 2015).
- Dadure C, Chrystelle S, Dalens BJ, Capdevila X (2014) Regional anesthesia in Milller RD, Eriksson LI, Fleisher LA,Kronish JP, Young WL (eds.). In: Paediatric Anesthesia. Miller’s anesthesia (8th ed). Library of Congress Cataloging-in-Publication Data, USA Pg no: 2706-2727.
- Ross AK, Bryskin RB (2011) Regional Davis PJ, Cladis FP, Motoyama EK (eds.). In: Smith’s Anesthesia for Infants and Children (8th ed). Philadelphia, Elsevier Mosby Pg no: 474-476.
- Franklin AD, Lorinc AN, Shotwell MS, Greene EB, Wushensky CA (2015) Evaluation of the skin to epidural and subarachnoid space distance in young children using magnetic resonance Reg Anaesth Pain Med 40: 245- 248.
- Uemura A, Yamashita M (1992) A formula for determining the distance from the skin to the lumbar epidural space in infants and children. Paed anest 2: 311-341.
- Gurrici S, Hartriyanti Y, Hautvast JG, Deurenberg P (1998) Relationship between body fat and body mass index: difference between Indonesians and Dutch Caucasians. Eur J Clin Nutr 52: 779-783.
- Wang J, Thornton JC, Russell M, Burastero S, Heymsfield S, et al. (1994) Asians have lower body mass index (BMI) but higher percent body fat than do whites: comparisons of anthropometric measurements. Am J Clin Nutr 60: 23-28.
- Tan SH, Teo EC, Chua HC (2002) Quantitative three-dimensional anatomy of lumbar vertebrae in Singaporean Asians. Eur Spine J 11: 152-158.
- Hasan MA, Howard RF, Lioyd-Thomas R (1994) Depth of epidural space in Anaesthesia 49: 1085-1087.
- Bösenberg AT, Gouws E (1995) Skin-epidural distance in children. Anaesthesia 50: 895-897.
- Mavrych V, Bolgova O, Ganguly P, Kashchenko S (2014) Age related changes of lumbar vertebral body morphometry. Austin J Anat 1: 1014.
- Wu HT, Schweitzer ME, Parker L (2005) Is epidural fat associated with body habitus? J Comput Assist Tomogr 29: 99-102.
Citation: Tantri AR, Perdana A, Rahmi R (2017) The Accuracy of Bosenberg Formula to Predict Skin-Epidural Distance in Malayan Pae- diatric Patients. J Anes Perio Manag 1: 001.
Copyright: © 2017 Tantri AR, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.