*Corresponding Author:
Bogdan Diaconescu,
Carol Davila University of Medicine and Pharmacy of Bucharest, Romania
E-mail: bogdan.diaconescu@yahoo.com
Abstract
The rarity of the inguinal hernias is given by the sac content which can be an ovary, appendix or Meckel diverticulum. Also, a complication of the content can be encountered leading to a change in management. We present the case of an Amyand’s hernia with large defect managed with classic mesh alloplastic repair and developing a rare postoperative early complication.
Keywords
Amyand; Inguinal hernia; Postoperative hydrocele; Rare hernia
Introduction
Inguinal hernias are the most often encountered parietal pathology of the adult. Hernias with particular content like ovaries, appendix, Meckel’s diverticulum are quite rare and some of them require special attention regarding surgical treatment and management of postoperative complications. We present the case of a patient presented to the Emergency Department with a voluminous inguinal hernia and the subsequent treatment and complications.
Case Presentation
A 57-year-old male patient presented to the Emergency Department for constipation and abdominal pain, symptoms that started approximately 6 years ago and aggravated in the previous 2 weeks prior ED presentation. The patient reported a history of arterial hypertension, atrial fibrillation and an ischemic stroke 5 years ago with a 2 out of 5 left brahio-crural motor deficit, all being controlled with specific oral medication. On physical examination, the patient is normotensive and with a SpO2 of 98% on breathing air. The heart sounds are irregular and the heart rate is less than 100 bpm. The abdomen is slightly distended and moderately diffusely painful without tenderness or guarding. On genital examination the patient presents extremely enlarged right hemiscrotum with bowel detected on palpation, slightly painful, not reducible, without signs of strangulation. The patient presents no other noteworthy modifications on physical examination.
Investigations
The ultrasound examination confirmed the right hernia containing bowels with no altered parietal perfusion and no free fluid in the sac. The measured hernia neck was 35mm. X-rays showed no alterations of the thoracic organs or abdominal free air-fluid levels. The abdom- inal CT-scan revealed a voluminous right hernia sac (131/157/250 mm) containing small bowel loops, cecum and ascending colon (Fig- ures 1-4) without other modifications. Lab values were normal.

Figure 1: Coronal CT scan.

Figure 2: Sagital CT scan.
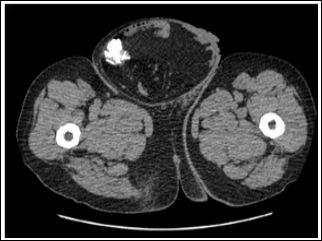
Figure 3: Transverse CT-scan.

Figure 4: 3D reconstruction of CT-scan.
After investigations were done, we excluded pathologies consid- ered for differential diagnosis like femoral hernia, testicular tumors, hydrocele or varicocele.
Management
The patient was proposed for surgery under general anesthesia. After preoperative evaluation, thromboprophylaxis and antibioprophylaxis were administered. The patient was placed in dorsal decubitus, the operative fields were placed and oblique inguinal incision with scrotal extension was made (Figure 5).

Figure 5: Intraoperative findings.
After entering the inguinal canal and hernia sac was opened a complete evaluation of the incarcerated organs was made (Figure 6).

Figure 6: Hernia sac content.
The case was classified as type I Losanoff and Basson classification and after the content reduction into the abdominal cavity and testicular fixation to the scrotum (not to torsion postoperatively) a 15x15cm polypropylene mesh repair was made and retro funicular closure of the external aponeurosis fascia and aspirated drainage of the residual cavity. The patient was discharged 3 days postoperative without immediate complications. At one-month follow-up he presented with enlarged right hemiscrotum and an early relapse was suspected. The ultrasound revealed voluminous hydrocele and a Lord procedure was performed in the same admission without any complications during postoperative period.
Discussion
In 1735, with 5 years before his death, Claudius Amyand operated an acute appendicitis of an 11-year old boy through a right inguinal hernia sac [1]. The reported incidence of Amyand’s hernia is approximately 1%, being more frequent on young boys due to persistence of peritoneo-vaginal canal [2]. Recently there was a classification proposed by Losanoff and Basson [3] in 2007 describing appropriate management of Amyand’s hernia based on the presence and grading of inflamed appendix into the sac (Table 1). Acute appendicitis into hernia sac is even rare entity appearing approximately 0.1% into some studies [4].
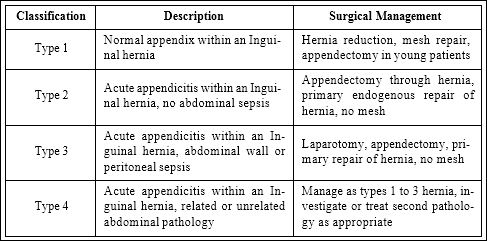
Table 1: Losanoff JE, Basson MD classification.
Conclusion
Amyand’s hernia is a rare form of inguinal hernia frequently encountered after herniotomy. Preoperative diagnosis must be completed with imagistic studies in order to exclude appendiceal inflammation and to adapt the management which should be guided by the presence of local sepsis and dimensions of the defect.
References
- Cárdenas AM, Valencia CF, Escárrega VH, Campos AC, Muniz EN, et al. (2015) Amyand hernia: Case report and review of the literature. Ann Med Surg (Lond) 4: 113-115.
- Ivashchuk G, Cesmebasi A, Sorenson EP, Blaak C, Tubbs SR, et (2014) Amyand’s hernia: A review. Med Sci Monit 20: 140-146.
- Losanoff JE, Basson MD (2007) Amyand hernia: What lies beneath a proposed classification scheme to determine management. Am Surg 73: 1288-1290.
- Green J, Gutwein LG (2013) Amyand’s hernia: A rare inguinal her- J Surg Case Rep: rjt043.
- Obney N (1956) Hydroceles of the testicle complicating inguinal Can Med Assoc J 75: 733-736.
Citation: Bratu MR, Balmes B, Diaconescu B (2020) Rare Complication after Amyand’s Hernia Repair-Case Presentation. J Emerg Med Trauma Surg Care 2: 008.
Copyright: © 2020 Bratu MR, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and re- production in any medium, provided the original author and source are credited.