*Corresponding Author:
Laura Morales-Ramírez,
Radiation Oncology Department, Instituto Nacional de Cancerología, Bogotá, Colombia
Tel: +57 3113093261
Email: lauramsrz12@gmail.com
Abstract
Neuroblastoma is the most frequent extracranial solid tumor in the pediatric age and radiotherapy is one of its pillars of treatment especially in high-risk patients. In order for this therapy to be provided effectively, it requires precision and reproducibility, so it is necessary for patients to be as still as posible for a period of time that varies between approximately 10 to 25 minutes, which is why the use of immobilizers and anesthesia are often required in these pediatric patients. Although anesthesia is a safe procedure, it is still an additional intervention, for this reason, recreational alternatives have been sought so that children are calmer in the face of Radiation therapy and can be treated without additional medical interventions. This is the case of a 3-year-old patient with a diagnosis of high-risk neuroblastoma who under went consolidation treatment with radiotherapy, due to logistical difficulties there was no availability of anesthesia, so it was decided to decorate the patient’s immobilizer to achieve that she was still and quiet in the treatment room. The result of this strategy was successful, the patient was much more comfortable and less fearful of the treatment, like her parents and was able to complete her treatment without anesthesia.
Introduction
Radiation therapy plays a fundamental role in the consolidation phase of patients with high-risk neuroblastoma [1]. In order for this treatment to be safe and accurate, it is necessary for patients to be as still as posible because movement can cause not only treatment failures but also additional toxicity [2], this becomes a challenge especially in younger children. Not only because of their youngage but because both patients and their parents are subjected to a high level of stress, causing that the perception of radiotherapy treatment may not be positive [3], this is even more marked in pathologies such as neuroblastoma where 89 % of cases occur before 5 years of age [4], it is for this reason that Immobilizers should be used and anesthesia is often necessary to be able to provide the treatment safely [5]. Even so, anesthesia is still an additional procedure that requires preparation, subsequent care and in some opportunities there may be difficulty in its availability. Recognizing this problem, different strategies have been created to make the treatment less frightening, one of these strategiesis the use of custom immobilizers and masks for each pediatric patient.
Case Report
This is the case of a 3-year-old patient who started with vomiting, diarrhea and abdominal pain, so an abdominal ultrasound was performed and an abdominal mass was reported, then a mass biopsy was performed that reporteda poorly differentiated neuroblastoma of non favorable histology. Additionally, a Positron Emission Tomography-Computed Tomography (PET-CT) was taken and metastatic involvement was ruled out. With these characteristics it was decided to initiate management with a protocol for high-risk neuroblastoma with neoadjuvant chemotherapy. Subsequently, the surgery was performed, managing to resect 20% of the lesion, then the patient was transplanted and finally referred to consolidation with radiotherapy. The patient was evaluated in the radiotherapy department and after being examined it was defined to schedule for external radiotherapy with Intensity-Modulated Radiation therapy (IMRT) for a dose of 21 Gy with subsequent boost up to 36 Gy. It was clearly explained to the parents what the radiotherapy consists of and the posible risks of the treatment, emphasizing the importance of being still during the treatment and the possibility of needing anesthesia, so that same day the patient was referred for evaluation by the anesthesiologist. Unfortunately for the day that the simulation CT had been scheduled it was not possible to have availability of the anesthesiology group, it is for this reason that it was decided to resort to other strategies and the patient was mentioned for the first time that there was the possibility of decorate her immobilizer, the reaction obtained was positive and it was possible to perform the simulation CT without problems. A thoracic immobilizer and a pelvic immobilizer were made, which were subsequently decorated with non-toxic water-based paint, paper and school glue with the design and colors chosen by the patient figure 1. A treatment plan with Volumetric Modulated Arc Therapy (VMAT) was approved (Figure 2), even though each sesión had a duration of about 9 minutes, in addition to these it was defined that inter-daily images of Kv would be taken as an IGRT strategy which added about 6 min to the sessions including the set-up, for which the duration of each treatment was between 9 and 16 minutes in which the patient should remain immobile.
On the day of the start of radiotherapy the patient was shown her immobilizer, the patient was happy and even excited to put on her immobilizer for the first time, a positive perception was also found in the patient’s parents. The patient was able to complete all of her treatment without any sedation or anesthesia, staying calm in each of the sessions.

Figure 1: Personalized immobilizer: The patient in treatment position with her immobilizer, frontan and lateral view.
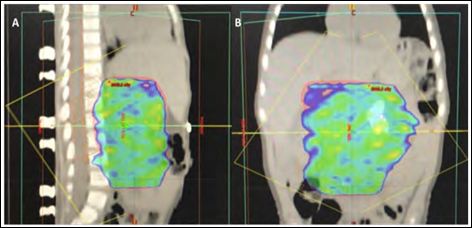
Figure 2: VMAT treatment plan: (A) latteral and (B) frontal view.
Discussion
Neuroblastoma is the most common extra creaial solid tumor in children [1] and has its highest incidence before 5 years of age [4] and although radiotherapy is essential in the consolidation of highrisk patients [1], it is a treatment that can cause anxiety for different reasons such as previous experiences with other treatments, having to remain alone in the treatment room or requiring them to remain still for significant periods of time [3].
Because radiotherapy requires great precision to be effective and have a lower chance of affecting neighboring structures [2] a commonly used tool for pediatric patients to main immobile during treatment is sedation or anesthesia that although it is quite effective and safe, it is still an additional intervention that needs preparation and post-treatment monitoring [5]. For this reason, different types of non-medical interventions have been sought to allow both patients and their parents to be calmer in the face of treatment [6,7]. The intervention used in this patient was to decorate her treatment immobilizers to her liking, thus allowing her to be much more comfortable and less anxious, especially during the first fraction of treatment as reported by other groups that use this same strategy [8]. This makes sense if we take in to account the systematic reviewç by O’Connor et al., where they conclude that therapeutic play, particularly the preparation of the procedure through play, seems to be a useful starting point for Interventions to reduce psychological distress in pediatric patients receiving radiation therapy [6].
Conclusion
The treatment of pediatric patients is a challenge not only academic but also emotional, since both children and their parents are under a great stress load, so the use of measures that can make a treatmen such as radiotherapy less frightening and more enjoyable is extremely valuable, that is why in cases like our patient’s it is important to look for other psychological, interactive or play full interventions that serve as an alternative to anesthesia, such as the Personalized decoration of immobilizers.
References
- Smith V, Foster J (2018) High-Risk neuroblastoma treatment re- Children 5: 114.
- De Ruysscher D, Niederman G, Burnet NG, Siva S, Lee AWM, et al. (2019) Radiotherapy toxicity. Nat Rev Dis Primers 5: 13.
- Kreitler S, Krivoy E, Toren A (2012) Psychosocial aspects of radio-therapy in pediatric cancer patients. In: Kreitler S, Ben-Arush MW, Martin A (eds.). Pediatric psycho-oncology: psychosocial aspects and clinical interventions (2nd edn). Wiley, New Jersey, USA. Pg no:328.
- Heck JE, Ritz B, Hung RJ, Hashibe M, Boffetta P (2009) The epide- miology of neuroblastoma: A review. Paediatric and Perinatal Epi- demiology 23: 125-143.
- McFadyen JG, Pelly N, Orr RJ (2011) Sedation and anesthesia for the pediatric patient undergoing radiation Curr Opin Anaes- thesiol 24: 433-438.
- O’Connor M, Halkett GK (2019) A systematic review of interventions to reduce psychological distress in pediatric patients receiving radi- ation Patient Educ Couns 102: 275-283.
- Angström-Brännström C, Lindh V, Mullaney T, Nilsson K, Wick- art-Johansson G, et al. (2018) Parents’ experiences and respons- es to an intervention for psychological preparation of children and families during the child’s radiotherapy. J Pediatr Oncol Nurs 35: 132-148.
- Van Dongen JJ, Haasbeek CJ, Slotman BJ (2018) Personalized painted masks may help to make pediatric radiation treatment more tolerable PO-1093 Estro Radiotherapy and Oncology 127: 615.
Citation: Morales-Ramírez L, Álvarez-Londoño A, Guerrero-Lizcano E, Esguerra-Cantillo JA (2020) Personalized Radiation Therapy Immobilizers as an Alternative to Anesthesia in Pediatric Patients: Case Report. J Perina Ped 4: 008.
Copyright: © 2020 Morales-Ramírez L, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.