*Corresponding Author:
Yi Lv,
Department of Hepatobiliary Surgery, First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, PR China
Tel: +213661227298
E-mail: xjtusjsy@aliyun.com
Abstract
Objective: To explore the new strategy of pre-hospital emergency treatment for severe trauma, research the effect of the abdominal magnetic compression device to control fatal abdominal trauma bleeding, and seek effective and convenient methods for emergency trauma or emergency trauma rescue.
Methods: A total of 36 healthy female adult rabbits, weight 1.72.3kg, were evenly divided into the intervention group (n=18) and the control group (n=18). All the rabbits were made into modelling of abdominal trauma in the hepatic region, using the free-falling steel ball after heparinization and carotid artery intubation. Then the intervention group used the abdominal magnetic compression device on the dorsal and ventral side of the body, while the control group received no intervention. We observed and recorded blood pressure curve, hemoglobin, bleeding volume and survival rate of the rabbits.
Results: The decrease of arterial pressure and bleeding in the intervention group was significantly lower than that in the control group (t = -2.772, P<0.05), and the hemoglobin level increased significantly (P<0.01). The survival rate of the intervention group was higher than that of the control group (P<0.05).
Conclusion: Usage of the abdominal magnetic compression device can quickly and effectively reduce the amount and speed of intra-abdominal hemorrhage, improve the survival rate of animals during the observation period, and create opportunities for transport and later surgery to stop bleeding.
Keywords
Closed abdominal trauma; Hemorrhagic shock; Intra-abdominal pressure; Magnetic abdominal compression device
Introduction
Deaths caused by various traumas are still serious public health problems, which not only seriously damage people’s lives, but also cause a huge economic burden [1]. Closed abdominal trauma is a common emergency in surgery. It can be seen in falls, impacts, knocks, crushing, trampling, etc. It has been widely valued due to rapidly progress and high mortality rate which caused by the frequent injury of multiple organs damage [2-4]. Statistics show that deaths due to trauma account for 10% of the total deaths each year. Trauma meets the conditions of serious social problems, 5.8 million people dying every year and 8.4 million being expected in 2020 [5]. Researches aimed at controlling internal bleeding in first aid of battlefield trauma are also a hotspot. Liver, spleen, kidney and mesenteric blood vessels are rich in blood flow and complex in structure. Surgeries could not intervene so properly that the treatment rate is pessimistic because of various damages, including ruptured parenchymal organs, omental mesangial damage and combined abdominal organ damage, could lead to hemorrhagic shock and excessive blood loss. Study showed [6,7] that the increasing of intra-abdominal pressure can reduce the velocity of intra-abdominal bleeding effectively. However, the compression bandage may lead to secondary damage of the accompanying fracture. The compression elastic abdominal band is effective only when abdominal distension occurs. The dorsal and ventral magnetic compression device is dexterity, which could support abdominal cavity during injury. It also has strong magnetic force and obvious compression effect. When the abdominal cavity swells, due to blood accumulation in the later period, the magnetic force could automatically weaken, which can prevent excessive pressure from affecting breathing. The purpose of this study was to establish a model of closed abdominal trauma in rabbits and observe the changes in the intra-abdominal hemorrhage of rabbits after applying magnetic abdominal pressure bands, so as to provide a theoretical basis for pre-hospital emergency measures for patients with closed abdominal injuries.
Materials and Methods
Research objects
A total of 36 healthy female adult rabbits, weight 1.7-2.3kg, were evenly divided into the intervention group (n=18) and the control group (n=18). The experimental animals were provided by the Animal Experimental Center of Xi’an Jiaotong University. The experiment complies with the relevant regulations on the ethics of laboratory animals of Xi’an Jiaotong University, and the ethics approval number of laboratory animals is No. 2019-1265.
Preparation of animal models
Fasting for solid and liquid in 12 hours before surgery. All animal models were anesthetized with 3% pentobarbital 1ml/kg and took supine position, fixing the limbs. Other preoperative preparations including shaving, sterilization and draping were completed. After carotid artery was cannulated and bladder was evacuation, the BL-420A biological function experimental system was used to monitor the changes in blood pressure. Heparins (12500U, 1ml/kg) were injected intravenously for heparinization. After the blood pressure has stabilized, fixed the impact device directly above the rabbit abdomen and the upper edge of the drop point should be aligned with the intersection of the right rib midline and the lower rib edge. Free ball was dropping at the height of 100 cm, and rabbits were quickly hit three times successively (Figures 1 and 2).
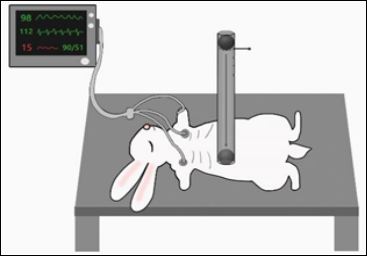
Figure 1: Schematic diagram of the rabbit abdominal closed injury model.

Figure 2: A: Schematic diagram of magnetic compression; B: Implementation of magnetic compression (a: a reel-like elastic band compressed on the abdomen; b: dorsal magnet).
Implementation of magnetic compression
After the impact, the intervention group applied a magnetic compression device immediately on dorsal and ventral side of the body, and fixed it to the abdomen of the rabbit. The main body of the dorsal and ventral magnetic compression device of the body was an independent reel-like device. The two axes were rod-shaped NdFeB materials, which were connected by an elastic band. The two shafts attracted the ventral magnets and pull the elastic band. The elastic band contracted, providing pressure to the abdomen in all directions. We controlled the abdominal pressure by adjusting the length of the elastic band between the two shafts. When the pressure was beyond limitation, the elastic band pull the two shafts to cause displacement, the elastic band between the two shafts became longer, and the abdominal pressure became smaller. (If you want to adjust the size of the magnetic force, you can only go through the bottom plate of the back. Our current method is to roll up several layers of elastic bands through the magnetic rod. When the pressure is beyond limitation, the magnetic rod rolls and releases a part of the elastic band. In this way, the elastic bands between the two magnetic rods become longer. The longer the pressure is, the smaller the applied pressure will be. If the dorsal magnetic force can be adjusted, the whole process will be more precise and smoother). The application of abdominal magnetic compression device on the dorsal and ventral side of the body will increase 1-1.5 times of bladder initial pressure (up to about 10mmHg). The application of the device can increase the intra-abdominal pressure and avoid affecting the respiratory system simultaneously. The control group did not intervene. After 90 min, with reducing the intravascular pressure and taking the midline incision of the abdomen, we dipped the blood in the abdominal cavity with gauze and weighed to calculate the amount of bleeding in the abdominal cavity.
Observation index
We observed the survival rate of rabbits at various stages after modeling. The dynamic change curve of rabbit blood pressure was drawn after modeling and the survival rates were counted at 30, 60, and 90 minutes for comparison between groups. Blood samples of jugular vein and carotid artery were taken as required 45 minutes after modeling. After 90 minutes, the rabbits were killed, and intra-abdominal blood samples were collected.
Statistical methods
SPSS18.0 software was used for data analysis, and the experimental data was expressed as deviation. Differences between count data groups were tested by chi-square test, and if the predicted frequency was less than 5, Fisher test was used. The difference between the measurement data groups was analyzed by one-way ANOVA, which was in accordance with the normal distribution and the variance was tested by two independent samples t-test, otherwise the Wilcoxon test was used. Take P<0.05 as the standard of significant difference.
Results
Changes in bleeding volume and haemoglobin
After animal closed abdominal trauma model was built, we ob- served that the bleeding volume of the intervention group was sig- nificantly reduced compared with the control group (P<0.05), and the hemoglobin level was also distinctly higher than the control group (P<0.01) (Table 1).
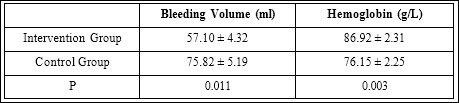
Table 1: Bleeding volume and Hemoglobin levels.
Changes in blood pressure
We observed that blood pressure began to fall rapidly, and contin- ued to decrease after a brief recovery until blood pressure could not be measured in this animal model (Figures 3 and 4). In the intervention group, 30min, 60min, and 90min arterial pressure dropped significant- ly lower than that in the control group (Table 2). The 30min, 60min and 90min survival rates of the intervention group were significantly higher than those of the control group (Table 3), The differences were statistically significant (P<0.05).

Table 2: Arterial Pressure Dropping Levels (mmHg).
Discussion
Closed abdominal trauma is complicated, often accompanied by substantial abdominal organ damage, and easy to induce hemorrhagic shock. Most patients have a critical condition along with changeable vital signs and complications such as shock and coma. Effective medical filed intervention could provide opportunities for transport and later surgical hemostasis, which could also reduce mortality and disability significantly. Despite the numerous medical managements for abdominal trauma [8], cumbersome operation and harsh conditions still limit the effect of emergency treatment, causing secondary injury frequently. Current first aid treatments have obvious shortages and are not completely suitable for patients in the first place or on their ways to the hospital, where many patients with intra-abdominal hemorrhage undergo few special treatments and die of excessive blood loss. Therefore, a device which could increase the intra-abdominal pressure through intelligent adjustment before sending to the hospital and effectively slow the internal bleeding caused by fatal closed abdominal trauma is of great need. Meanwhile, the device is meant to reduce side injury caused by excessive abdominal compression, improving the survival rate and prognosis of patients with war or accident trauma.

Figure 3: Schematic diagram of experiment operation (A. Trans-arterial intubation; B. Preparation of experimental model; C. Intervention group display; D. Control group display; E. Abdominal bleeding display).
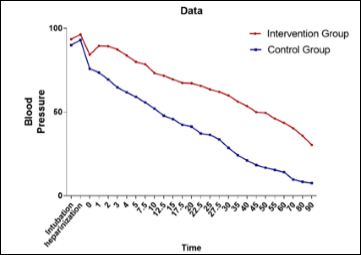
Figure 4: Time-Dependent Changes of Blood Pressure Levels (Blood pressure value of intervention group is significantly higher than that of control group at each time point).
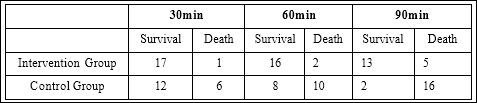
Table 3: Comparison of the difference between rabbits survival number of groups.
We used a special magnetic abdominal compression device, which is easy to operate and fix, to increase the intra-abdominal pressure. We found that at the end of 30min, 60min, 90min, the survival rates of the intervention group, using a special magnetic abdominal compression device, were all significantly higher than that of the control group, so did the peripheral blood hemoglobin. Moreover, the bleeding volume of the intervention group was also lower than that of the control group. The blood pressure curves showed the same trend in both intervention group and control group: a rapid decrease in blood pressure was observed after a short period of time after modeling, and then entered a plateau or a transient increase. After that, the blood pressure eventually continued to decrease until death. It suggested that under the condition of fatal closed abdominal trauma, the application of special magnetic abdominal compression device could significantly reduce the amount and rate of bleeding in the abdominal cavity. In addition, the loss of blood volume was basically consistent with hemoglobin level and blood pressure in jugular vein, which indicated that life signs could be reflected by monitoring blood pressure after closed abdominal trauma.
The advantage of the special abdominal magnetic compression device is fast fix, convenient in carriage and people will comprehend quickly with simple instructions. It is suitable for first aid and transport under harsh conditions. Compared with the traditional treatment plan for closed abdominal trauma (especially its usage in first aid), the special abdominal magnetic compression device greatly could shorten the operation time and reduce intra-abdominal bleeding effectively. Moreover, traditional compression bandage may cause secondary injury. Along with the increasing pressure, non-adjustable traditional compression bandage could also affect the compliance of the lungs. The impact on the digestive system and other multiple systems cannot be ignored. According to research in recent years, there may be a close relationship between intra-abdominal hypertension (IAH) and abdominal cavity syndrome (ACS). ACS is characterized by increased end-expiratory pressure and hypoperfusion secondary to low cardiac output.
Severe pulmonary insufficiency with venous reflux disorder and hyper inspiratory peak with hypercapnia. This must be treated early in surgery. Patients with prolonged untreated elevations in intra-abdominal pressure commonly manifest inadequate perfusion and subsequent organ failure [9]. Preexisting comorbidities, such as chronic renal failure, pulmonary disease, or cardiomyopathy, play an important role in aggravating the effects of elevated intra-abdominal pressure. Elevated intra-abdominal pressure contributes to kidney dysfunction, which could induce both hemodynamic alterations and renal tubular dysfunction [10]. Some studies reported that after a period of operating, traditional compression bandage may endanger life signs of patients [10-12].
Our dorsal and ventral magnetic compression device, taking full advantages of magnetic, is meant to realize fully automatic intelligent adjustment in its supporting magnetic surgery environment. It also avoids causing harm to patients due to unreasonable abdominal high pressure. However, it should be noted that the method of increasing intra-abdominal pressure is only used in first aid, as an emergency treatment method, to delay intra-abdominal hemorrhage, which cannot stop bleeding and have a radical therapeutic effect. In the case of multiple organ damage or accompanied with large blood vessels rupture, the effect would be limited. Once the magnetic abdominal compression device has delayed the amount and speed of abdominal bleeding, prompt surgery is still the ultimate and only option for patients.
At present, the device is not accurate enough to adjust the magnetic force, which means pressure applied to the abdomen may float within a certain range. The optimal range of abdominal compression and its impact on major systems still needs more experimental support. We will continue to develop a more accurate magnetic device for the abdomen, which can control various units more flexible and accurate, according to the vital signs its detected. We will keep on devoting to magnetic surgery research, making full use of its simplicity, high efficiency and celerity, and contributing to the promotion of medical development.
Conclusion
According to our results, the application of magnetic abdominal compression device increases the intra-abdominal pressure of patients in the situation of acute closed abdominal trauma. It could effectively reduce the amount and speed of intra-abdominal hemorrhage, improve the survival rate during the observation period, and create opportunities for transport and post-operative hemostasis.
Funding
Military logistics research project (BZZ19J004).
References
- Soto JA, Anderson SW (2012) Multidetector CT of Blunt Abdominal Radiology 265: 678-693.
- El-Menyar A, Abdelrahman H, Al-Hassani A, Peralta R, AbdelAziz H, et al. (2017) Single Versus Multiple Solid Organ Injuries Following Blunt Abdominal World J Surg 41: 2689-2696.
- Bergeron E, Lavoie A, Belcaid A, Moore L, Clas D, et al. (2007) Surgical management of blunt thoracic and abdominal injuries in Quebec: a Limited J Trauma 62: 1421-1426.
- Hoppe IC, Kordahi AM, Lee ES, Granick MS (2015) Pediatric Facial Frac- tures: Interpersonal Violence as a Mechanism of Injury. J Craniofac Surg 26:1446-1449.
- Paun S, Beuran M, Negoi I, Runcanu A, Gaspar B (2011) Trauma–epidemiol- ogy: where are we today? Chirurgia 106: 439-443.
- Kasotakis G, Duggan M, Li Y, Dowd D, Baldwin K, et (2013) Optimal pres- sure of abdominal gas insufflation for bleeding control in a severe swine splenic injury model. J Surg Res 184: 931-936.
- Ahmadi-Noorbakhsh S, Azizi S, Dalir-Naghadeh B, Maham M (2012) Hyper- pressure Intraperitoneal Fluid Administration for Control of Bleeding after Liv- er Injury. J Surg Res 176: 559-566.
- Huseyin N, Hukum U, Keziban UK (2012) The Diagnostic Value of Intra-ab- dominal Pressure in Patients with Blunt Acute Abdominal Cukurova Med J: 37.
- Malbrain ML, Cheatham ML, Kirkpatrick A, Sugrue M, Parr M, et al. (2006) Results from the International Conference of Experts on Intra-abdominal Hy- pertension and Abdominal Compartment Syndrome. I. Definitions. Intensive Care Med 32: 1722-1732.
- Saleh NA, Aronson D, Khamaisi M, Khoury E, Awad H, et (2019) Increased Intra-abdominal Pressure Induces Acute Kidney Injury in an Experimental Model of Congestive Heart Failure. J Card Fail 25: 468-478.
- Pelosi P, Meinhardt JP, Caironi P, Quintel M, Gattinoni L (2001) Effects of Intra-Abdominal pressure on Respiratory Mechanics in healthy and injured Eur J Anaesthesiol 18: 21.
- Runck H, Schumann S, Tacke S, Haberstroh J, Guttmann J (2012) Effects of intra-abdominal pressure on respiratory system mechanics in mechanically ventilated rats. Respir Physiol Neurobiol 180: 204-210.
Citation: Lv Y, Song J, Liu S, Zhao C, Feng Y, et al. (2020) Magnetic Abdominal Com- pression for Controlling Internal Bleeding in Fatal Closed Abdominal Trauma in Rab- bitsan: Experimental Study. J Emerg Med Trauma Surg Care 2: 009.
Copyright: © 2020 Lv Y, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and re- production in any medium, provided the original author and source are credited.