*Corresponding Author:
Khairunnisa Che Ghazali,
Department of General Surgery, Miri Hospital, Sarawak, Malaysia
Tel: +60 133520785
Email: khairunnisacg@gmail. com
Abstract
Traumatic diaphragmatic hernia is a rare sequela following blunt abdominal trauma, which can also be a life-threatening condition. Subtle presentation may cause delay in diagnosis. However, respiratory distress itself can be a nonspecific presenting symptom in many other traumatic scenarios. Therefore, a high index of suspicion is necessary to make a diagnosis of diaphragmatic rupture, especially in the absence of pathognomonic radiographic findings. In recent times, an increasing number of successful laparoscopic repairs have been reported worldwide. We would like to share our humble first experience in one patient, who had a traumatic diaphragmatic hernia, presented with upper quadrant abdominal pain and treated with laparoscopic surgery.
Case Presentation
A 77-year-old man presented to the hospital after involving in a road traffic accident complaining of left upper quadrant abdominal pain. He was the car driver which collided with another car from the left. Post trauma, the patient sustained a brief period of loss of consciousness, pain at the left upper quadrant and left lower limb. He had no shortness of breath, no chest pain, and no other major injuries. Vital signs on arrival were stable. Respiratory and cardiovascular examination was unremarkable. There was tenderness over left upper quadrant of the abdomen on palpation.
Chest x-ray (Figure 1A) showed possible left diaphragmatic hernia, which was confirmed with a CT Thorax, Abdomen and Pelvis. Figure 1B showed presence of herniation of intra-abdominal content into the left thoracic cavity with left lung collapse and grade 2 splenic injury.
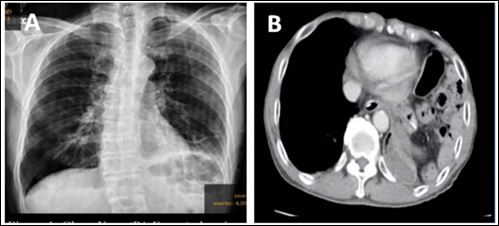
Figure 1: (A) CXR showed elevated left hemidiaphragm with bowel loop suspecting diaphragmatic hernia. (B) CT axial image confirming part of bowel herniated into the left thoracic cavity.
Hence, we decided for a laparoscopic diaphragmatic hernia repair. Patient was brought to the operating theatre after adequate resuscitation. Exploratory laparoscopy was performed. Left diaphragmatic defect measuring 4x4cm was found with part of the transverse colon, splenic flexure, small bowel, stomach and spleen seen herniating through the defect. A content of the hernia was brought down fully into the abdomen (Figure 2A&B). Left chest tube was inserted prior to closing of defect and the defect was repaired using Strata fix 2/0 continuous sutures (Figure 3A&B). Patient tolerated the procedure well. He was allowed home 5 days post operation.
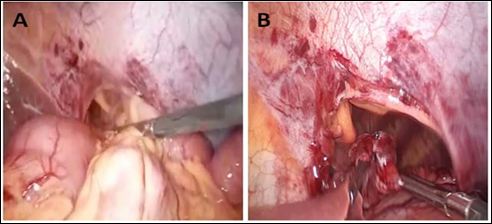
Figure 2: (A) Herniated organs being reduced into the abdominal cavity. (B) 4x4cm diaphragmatic hernia defect.
Discussion
Traumatic Diaphragmatic Hernia (TDH) can occur in both blunt and penetrating abdominal trauma. However, blunt abdominal trauma only accounts about 35% of TDH cases [1,2]. Most of the diaphragmatic hernia involves the left hemidiaphragm, about 80-90% as opposed to the right side [2,3], this is because the right side is protected by the liver.
High index of suspicion is necessary to make a diagnosis of TDH. Usually patient will be asymptomatic and physical examination may be unremarkable. It is still possible for TDH presented later in life with In this case, during assessment, complications of herniated organs including strangulation or perforated viscus had been ruled out prior repair. Then, the diaphragmatic defect was repaired using non-absorbable sutures. The diaphragmatic edges could be reapproximated without tension, hence primary repair was performed. Simple running, interlocking suture was used. In a case of failure to achieve tension-free repair, the use of synthetic mesh is advisable [1].
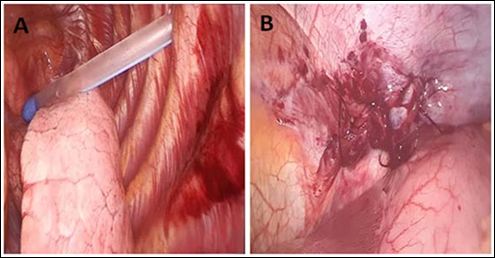
Figure 3: (A) Chest tube inserted into the left thoracic cavity under direct vision. (B) Hernia defect repaired using non absorbable suture.
complication from herniation. Diagnosis of TDH should be complimented with computed tomography as adjunct to plain radiograph in highly suspicious cases of thoracoabdominal injury [1,2]. Initial imaging may miss diaphragmatic hernia by 30-50% of acute cases [2,3].
Diagnostic laparoscopy plays a dual role, as diagnostic and therapeutic. Diagnosis of diaphragmatic rupture nearly 100% via laparoscopy [2,3]. It also allowed exploration of the whole peritoneal cavity together with diaphragm evaluation via a keyhole surgery. Laparoscopy is preferred than thoracoscopy as thoracoscopy only allow single hemidiaphragm evaluation and difficulty in assessment of herniated organ. Laparoscopy allows contents to be reduce easily and allows better assessment of the organs [4]. Other than that, the advantage of minimally invasive surgery such as less post-operative pain, early recovery, and decrease hospital stay as compared to open surgery [5]. However, in a study by Paul et al., there was no significant difference in term of post-operative morbidity such as pneumonia, deep vein thrombosis, myocardial infarction or sepsis between traditional open approach versus laparoscopic [5].
Conclusion
Traumatic diaphragmatic hernia is not only uncommon but can also sometimes be under diagnosed. High index of suspicion and prompt surgery needed to avoid mortality risk. Laparoscopic repair is a safe and effective treatment in traumatic diaphragmatic injury.
References
- Shamim AA, Zuberi MM, Tran D, Fullum T (2020) Laparoscopic re- duction and repair of acute traumatic diaphragmatic hernia: A video Laparosc Endosc Robot Surg 3: 22-25.
- Xenaki S, Lasithiotakis K, Andreou A, Chrysos E, Chalkiadakis G (2014) Laparoscopic repair of posttraumatic diaphragmatic rupture. Report of three Int J Surg Case Rep 5: 601-604.
- Nguyen P, Davis B, Tran DD (2017) Case report laparoscopic repair of diaphragmatic rupture : A case report with radiological and surgi- cal Case Rep Surg 2017.
- Ağalar C, Benli S, Egeli T, Ozbilgin M, Basara I (2017) Laparoscopic repair of delayed traumatic diaphragmatic hernia with mesh. Trau- ma Acute Care 2:
- Paul S, Nasar A, Port JL, Lee PC, Stiles BC, et al. (2012) Compar- ative analysis of diaphragmatic hernia repair outcomes using the nationwide inpatient sample Arch Surg 147: 607-612.
Citation:Othman A, Ngu V, Ghazali KC, Hamidi AJA, Aimanan K, et al. (2020) Lapa- roscopic Repair of Traumatic Diaphragmatic Injury in a District Hospital: Our Humble Experience in a Northern Region of Sarawak. J Case Repo Imag 4: 014.
Copyright: © 2020 Othman A, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
