*Corresponding Author:
Sarv Priya,
Department of Radiology, University of Iowa Hospitals & Clinics, Iowa, USA
Tel: +1 3195125404
Email: sarv-priya@uiowa.edu
Clinical Images
A 19-year-old female with Crohn’s disease (diagnosed at 11 years of ages) presented with history of lower abdominal pain, night sweats, urinary urgency, and urethral burning sensation. A month ago, she complained of alternating right and left flank pain and per urethra discharge of hard stool pellets followed by more liquid stool during urination. She denied pneumaturia. Magnetic Resonance Enterography (MRE) was requested to evaluate for exacerbation of Crohn’s disease. A non-contrast CT revealed soft-tissue between terminal ileum and dome of bladder (Figure 1), raising concern for fistula formation. MRE revealed wall thickening of terminal ileum and ileocecal junction with diffusion restriction and post-contrast enhancement (Figure 2). Findings were consistent with active Crohn’s disease. Additionally, a serpiginous T2 hyperintense tract (Figure 1) was seen extending from the small bowel loop towards the bladder dome. On cine images, a linear hypointense jet was clearly seen running from superior bladder inferiorly, indicating flow of intestinal contents through an enterovesical fistula into the bladder (Video-1 and Figure 3). The formation of the fistula was likely due to transmural inflammation affecting terminal ileum resulting in breakthrough of the wall and eventual communication with urinary bladder located in its proximity. The enterovesical jet may be confused with urinary jets. Urinary jet is a normal phenomenon and can be observed in normal individuals. However, a urinary jet will be seen arising from ureteral orifice, whereas the jet in entero-vesical fistula typically arises from bladder dome. MRE provides advantage over computed tomography in localizing enterovesical fistula without radiation exposure.
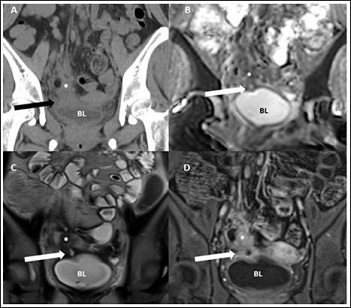
Figure 1: Entero-vesical fistula.
Non-contrast coronal CT (A) image shows soft-tissue between terminal ileum and bladder dome. Coronal ADC (B), HASTE (C) and post-contrast (D) images show presence of fistulous connection between terminal ileum and bladder dome (arrow).*- Terminal ileum; BL- Bladder.
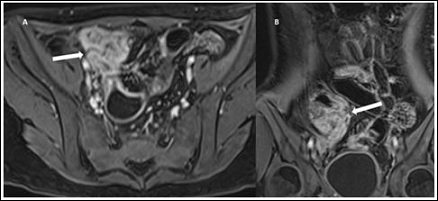
Figure 2: Terminal ileal involvement in Crohn’s disease.
Post contrast magnetic resonance angiography axial (A) and coronal (B) images show enhancement of terminal ileum and ileo-cecal junction (arrow).
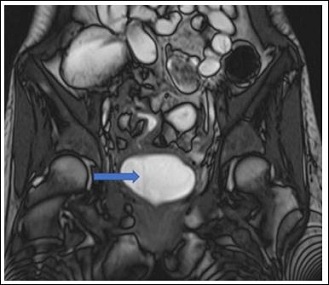
Figure 3: Cine image.
Still frame from coronal cine series clearly shows a hypointense jet in bladder arising from a bowel loop (arrow) confirming enterovesical fistula (also shown in the video).
Citation: Priya S, Kao SC (2019) Jet Phenomenon in Enterovesical Fistula from Crohn’s Disease. J Case Repo Imag 4: 009.
Copyright: © 2019 Priya S, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
