*Corresponding Author:
Azuonwu Obioma,
Department of Medical Laboratory Science, Rivers State University, Port Harcourt, Nigeria
Tel: +234 8035519688
E-mail: bimajacobs@yahoo.co.uk
Abstract
The study will attempt to investigate the impact and spatial hematological variations among subjects infected with Hepatitis B Virus in some Niger Delta Communities. A total of 1000 subjects of age ≥15 were recruited through convenience random sampling research design. Three milliliters of whole venous blood was collected from the anticubital vein of each subject and were dispensed into an Ethyl Diamine Tetra Acetic Acid (EDTA) bottle. The blood was used to screen for the presence of surface antigen of Hepatitis B virus and also the Packed Cell Volume (PCV), Hemoglobin (Hb) and White Blood Cell (WBC) count were determined using standard laboratory diagnostic techniques. The result of the study recorded 14% prevalence rate of HBsAg among the screened subjects; 40.7% of which were males and 59.3% were females. The mean WBC count of the sero-positive subjects were 8.73x108/l while that of the negative subjects were 6.37x108/l, the mean Haemoglobin (Hb) value of the infected subjects were 10.48 g/dl, while that of the non-infected subjects were 11.54 g/dl, even as the mean PCV of the sero-positive subjects were 31.56% while that of the sero-negative subjects were 34.62%. The frequency of occurrence of HBsAg among the different age groups showed that the age group of 25-34 recorded a higher percentage of HBsAg infection with 34.3%; while age group of 45-54 recorded the least with 9.3% respectively. The need for continuous robust health awareness campaign, especially in the rural communities will be helpful towards reducing the trend, even as the provision of functional health care facilities with modern laboratory diagnostic tools would also facilitate prompt diagnosis and treatment outcome of the infection, in the limited resource regions of the world
Keywords
Hemoglobin concentration; Hepatitis B virus; Niger delta communities; Pack cell volume; Spatial variations; White blood cells
Introduction
Hepatitis refers to liver inflammation and may be caused by toxic agents, bacteria, drugs, viruses, autoimmune disorders or even circulatory or metabolic disorders [1]. Its viral causative agents include hepatitis, A, B, C, D and E. Hepatitis B is however the commonest and is more fatal of all [2]. In 2015, 1.34 million cases attributed to HBV were recorded worldwide [3]. Hepatitis B Virus (HBV) was discovered by Baruch Blumberg in 1963 in the blood of Aborigines in Australia [4]. It is a double-stranded enveloped DNA virus belonging to the family Hepadnaviridae [5]. Hepatitis B virus DNA, HBcAb, HBcAg, HBsAb, HbsAb, HbeAb and HBeAg are important serological markers of the virus in determining how severe the illness is, as well as in diagnosing the infection [6]. About 600, 000 persons die yearly as a result of HBV infection [7]. According to the WHO [3], 257 million persons (3.5% of the world’s total population) were estimated to be living with chronic HBV as Africa and the Western Pacific made up 68% of the infected population.
Its routes of transmission include sexual intercourse with an infected individual and contact with body fluid such as blood which is infected. The illness is mostly asymptomatic, however in some cases, symptoms may appear within 6 weeks to 6 months from infection [8]. Intravenous Drug Usage, tattooing, homosexuality, dental procedures as well as surgeries are some of the critical risk factors that may influence the spread of the virus [9]. Symptoms of the illness include stomach upset, fatigue, and fever, nausea, yellowing of the eyes and skin, lack of appetite as well as joint pain [10]. Occasionally, sero-positive HBsAg individually are asymptomatic and this may be challenging as the virus continues to spread and at the same time destroy the liver of an infected host. Nevertheless, it is therefore very important that proper diagnosis be carried out using specific markers other than the use of mere signs and symptoms as a basis for prognosis and diagnosis of the infection. The haematological and immunological state of HBV infected patients is often neglected in routine diagnostic investigations of those infected with the virus, especially in rural communities treatment centers, which tend to worsen the already health complication issues of the infected subjects. Hepatitis B is a viral infection of critical Public Health importance globally, though more prevalence rate is recorded among the developing communities probably due to poor health awareness campaign on personal hygiene and lack of functional health care infrastructure for prompt prognosis and diagnosis of the pathogen. Nevertheless, it is strongly believed that availability of functional health system and well trained health personnel would promote fast treatment of the infected subjects, even as well as curtail the wide spread of the infection in a reasonable and significant manner in a given locality. However, the potential infection of the liver by these viruses may lead to the inflammation of the liver, also known as liver cirrhosis. Nonetheless, in most rural communities within the Niger Delta region, little or no attention is paid to assay or investigate the impact and the association of Hepatitis B virus infection with respect to some hematological parameters of patients who visit the health facilities with myriads of signs and symptoms as such, there seems to exist a huge gap of information and communication in this direction of study, thus, the study would attempt to compare the hematological parameters of the HBsAg sero-positive and sero-negative subjects. Furthermore, an association would also be explored among the infected male and female subjects with respect to the impact of the virus on some hematological profile of the subjects respectively.
It is therefore, strongly believed that data generated from the study would stimulate much needed attention for government and relevant health agencies to consider the broad spectrum management strategy which would enhance the earlier detection of the virus and good treatment option outcome of the infection.
Methodology
Study location
Subjects for this study were drawn from Ahoada East Local Gov- ernment Area of Rivers State. It is located in the oil-rich Niger Delta region of Nigeria. Its population according to the NPC [11] is about 178,279 with the indegenes belonging to the Ekpeye ethnic nationali- ty. The occupations of the people include farming, trading and fishing.
Inclusion criteria
Subjects drawn for this study were persons of age ≥15 resident in Ahoada Local Government Area and willing to give an oral consent to partake in the study.
Exclusion criteria
Subjects who are less than 15 years were not allowed to participate and those who could not provide the consent to participate were also removed. The subjects must be a resident of the study location.
Ethical approval
The ethical approval was sought and approval was granted by the Rivers State Hospital Management Board ethical communitee, Port Harcourt.
Sample collection
A total of 1000 subjects were used in this study through conve- nience sampling research design. Three milliliters of whole venous blood was collected from the anticubital vein of each subject and were dispensed into an Ethyl Diamine Tetra Acetic Acid (EDTA) bottle with a proper mix, for haematological parameter assay (PCV, Hb and WBC cell count). They were stored at 4 ºC for analyses after the sep- aration of the blood cells was done using well effective centrifuge at 1500 rpm per minute for 3-5 minutes.
Experimental
Screening for HBsAg
Sera from all subjects were analyzed for hepatitis B surface antigen (HBsAg) using the commercially available Acon HBsAg test strips (Acon Laboratories, Inc. San Diego U.S.A). Manufacturer’s instructions were strictly adhered to. The Hepatitis B surface Antigen Rapid Test Strip (Serum) is a rapid chromatographic immunoassay for the qualitative detection of hepatitis B surface antigen in serum. The membrane is pre coated with antiHBsAg antibodies on the test line region of the strip. During testing, the serum specimen reacts with anti-HBsAg antibodies conjugated particles. The mixture migrates upward on the membrane chromatographically by capillary action to react with anti HBsAg antibodies on the membrane and generate a colored line. Kits used for the screening of HBV infection were interdem with the kits recommended by WHO for low income resource countries which Nigeria is inclusive.
Positive results
The presence of two distinct colored lines were observed. One line was observed in the control region (C) while another line was in the test region (T).
Negative results
The result was declared negative if there was one colored line on the control region (C) and there was no apparent colored line which appeared in the test region (T).
Invalid
The analysis was declared invalid if the control line failed to appear. Insufficient specimen volume and poor procedural techniques are the most likely reasons for false negative and positive results during the analysis.
Haematological Examination of Blood Samples
Estimation of haemoglobin concentration
The hemoglobin levels of collected blood samples were estimated using the cyanmeth-haemoglobin method [12]. Blood (0.02 ml) was diluted with 5.0ml of Drabkin’s reagent. After 10 minutes, the colour intensity of the solution was measured photometrically at 540 nm. Water was used as blank. The haemoglobin level was obtained from a calibration curve prepared with the aid of commercially available standards.
Determination of packed cell volume
The packed cell volume values were determined using the microhematocrit method [12]. The capillary tube was filled with homogenized blood (70mm long and 1mm wide) by capillary action leaving approximately 10 mm unfilled. The empty end was sealed with a plastic stopper. Centrifugation was carried out with haematocrit centrifuge (Microfield England) at 12,000rpm for 4 minutes. The packed cell volume was read using a haematocrit reader scale.
White blood cell count estimation
The white blood cell count was determined using an improved Neubauer (Assistant, Germany) counting chamber with Turk’s solution as diluent. Anticoagulated blood (0.02 ml) was diluted with 0.38 ml of Turks solution in a clean dry test tube. The improved Neubauer counting chamber was charged with the solution with a clean pipette. This was allowed to stand for five (5) minutes at room temperature. The principle is based on the fact that the glacia acetic acid content of the Turks solution destroys the red blood cell while the tincture of methylene blue stains the white blood cell which makes them more visible to be counted [13].
Results
The results of this study showed that of the 1000 subjects, 14% were HBsAg positive while 86% were negative (Figure 1). (Figure 2) shows the percentage distribution of the study subjects based on gender. 46.4% were males while 53.6% were females. Also, of the sero-positive subjects, 40.7% were males, while 59.3% were females. The mean WBC count of the subjects showed that, that of the sero-positive subjects was 8.73x108/l while that of the negative subjects was 6.37x108/l (Figure 3). (Figure 4) shows that the mean Haemoglobin (Hb) value of the infected subjects was 10.48 g/dl, while that of the non-infected subjects was 11.54 g/dl. Mean PCV of the sero-positive subjects was 31.56% while that of the sero-negative subjects was 34.62% (Figure 5). The frequency of occurrence of HBsAg among the different age groups was represented in (Figure 6). The figure shows that age group 25-34 recorded a higher percentage of HBsAg with 34.3%; while age group 45-54 recorded the least with 9.3%.
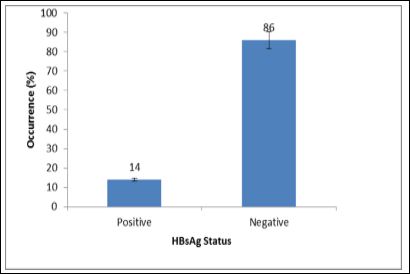
Figure 1: Percentage prevalence of HBsAg among the subjects.
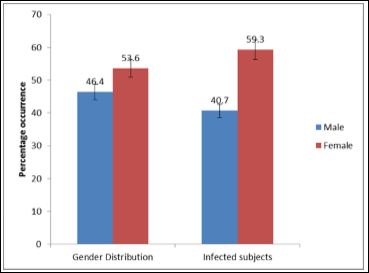
Figure 2: Percentage distribution of the collected samples and prevalence of HBsAg among the genders.
Discussion
The body’s response to illnesses affects the serological, clinical and haematological presentation of a pateint. This is because the ability of the immune system to fight infections determines how severe the illness will be [2]. The prevalence of HBsAg recorded in this study was 14%. This is closely related to the 13.6% obtained by Musa et al.[14] who carried out a similar study in Nigeria. However, the slight difference observed may probably be due to sample size and method of assay employed. Nonetheless, females had a higher prevalence rate of 59.3% while males made up 40.7% of the total prevalence. A study by Jeremiah and Tony-Enwin [15] carried out among University students reported a higher percentage among males than females. This difference may be attributed to the difference in location as the location of the present study is a rural area and often made up of females indulged in farming and other small scale businesses. Also, the higher percentage (53.6%) of females involved in this study compared with the 46.4% of male subjects may have probably contributed immensely to this increased prevalence, recorded among the female subjects. Furthermore, it is obviously no longer a big news that females are always more in number when compared to the number of female to male ratio in any gathering in our society, ranging from churches, schools, markets and even in ceremonies. Thus, the aforementioned factors may have accounted for the increase in female prevalence rate.

Figure 3: Mean WBC value of the subjects.

Figure 4: Mean Haemoglobin (Hb) value of the subjects.

Figure 5: Mean PCV value of the subjects.
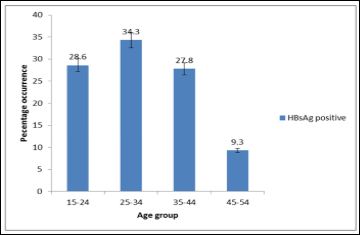
Figure 6: Percentage prevalence of HBsAg among the age groups.
The WBC count was higher in the infected individuals (8.73x108/l)) when compared with the uninfected individuals (6.37x108/l). This however, is antonymous to the study carried out by Ajugwo et al.,
[2] who recoreded lower WBC counts among infected subjects but in consonace with the study by Onwusuanya et al. [16] who reported higher WBC counts in sero-positive subjects. However, the importance of WBC count level can never be overemphesized as the cells served as the defence machanism in our system especially, during the abrupt of an epidemic outbreak, hence an increase in the white blood cell count among the infectd subjects are not suprising as these cells are potentially released to fight when a foreign body, otherwise known as antigen enters the host cell to cause a disease condition.
One of the critical function of haemaglobin is to transport oxygen round the tissues, organs and cells in our whole system. The cells or tissues that is starved of oxygen is as good as a dead cell, hence may not function effectively.
Haemoglobin concentration of the HBsAg sero-positive subjects was lower (10.48 g/dl) than that of the sero-negative subjects (11.54 g/dl). This is in agreement with the study by Ajugwo et al. [2] who reported lower Hb concentration (12.4 g/dl) of positive subjects compared with the control (15.4 g/dl). Also studies by Onwusuanya et al. (2017) [16] recorded lower Hb level which was also in consonance with this present study.
This study recorded a decrease in PCV in the sero-postive individuals that than of the sero-positve individuals. This finding is synonymous to the study carried out by Ajugwo et al. [2] who recorded a lower PCV value (37.2%) among HBsAg infected subjects than the uninfected subjects (45%). Onwusuanya et al.[16], also reprted lower Hb concentration compared with HBsAg negative individuals. Malnutrition, possible blood loss and well as infections have been linked to low PCV values [17]. According to Goldsby et al. [18], the presence of an infectious disease promotes the rise in WBC count because of the infiltration of inflammations to the site of infection. Several studies in Nigeria maintained that mutliple sex partners, intravenous drug use, sex at early age as well as homosexuality increases the risk and occurrence of most sexually-transmitted diseases such as HBV and HIV among youths [19,20].
Nonetheless, one strong outcome identified as weakness cum limitation in the study was that the researchers did not analyse and count the differential whilte blood cell count of the blood of the subjects, such as lymphocyte, monocyte, basophil and eosinophil, even as their staining reactions was not presented due to lack of fund. These would have also helped to improve the novelty of the study. However, further studies should consider these direction to enahnce the scope and novelty of the work. However, the study was not sponsored by any organistion hence, lack of grant was very instrumental to non expoundsion of the scope of work beyound self sponsorship financial capacity. Nonetheless, the above limiting factors were noted for further studies in these area in the nearest future.
Conclusion
This study highlights the need to investigate haematological parameters as a routine assay in HBV positive individuals, as this will go a long way in the survival of these individuals.The results of this study showed that of the 1000 subjects, 14% were HBsAg positive while 86% were negative. Also percentage distribution of the study subjects based on gender revealed that 46.4% were males while 53.6% were females. Also, of the sero-positive subjects, 40.7% were males, while 59.3% were females. The mean WBC count of the subjects showed that, that of the sero-positive subjects was 8.73x108/l while that of the negative subjects was 6.37x108/l Furthermore, the mean Haemoglobin (Hb) value of the infected subjects was 10.48 g/dl, while that of the non-infected subjects was 11.54 g/dl. Nevertheless, the mean PCV of the sero-positive subjects was 31.56% while that of the sero-negative subjects was 34.62% respectively.
As a means of prevention strategy of the spread of HBV, blood should be properly screened before tranfusion outcome. However, vaccines should be made available and individuals should be strongly encouraged to be vaccinated in good time, even as well as increase awareness advocacy on the risk factors of HBV infection in our rural communities across the globe would help to reduce the pandemic infection.
References
- Nester EW, Anderson DG, Roberts EC, Nester TM (2009) Microbiology a human perspective (6th edn) McGraw Hill: NY, USA pp: 606-608.
- Ajugwo AO, Ukaji DC, Erhabor TA, Adias TC (2015) Some Haematological Parameters of Symptomatic and Asymptomatic Hepatitis B Positive Patients Attending a Nigerian Tertiary British Journal of Medicine & Medical Research 7: 219-223.
- Chan M (2017) World Health Organization (2017). Global Hepatitis Report.
- Alter HJ, Blumberg B (1966) Further studies on a new human isopreciptin Blood 27: 297-309.
- Washington N, Allens S, Konemane JP, Procop OG, Schreckenberger P, et (2006) Koneman’s Colour Atlas and Textbook of Diagnosis Microbiology (5th edn) Lippincoh Williams and Wilkine: Philadelphia, USA pp: 1343-1372.
- Alberti A, Chemello L, Benvegnu L (1999) Natural history of hepatitis Journal of Hepatology 31: 17-24.
- World Health Organization (2001) Introduction of hepatitis B vaccine into Immunization Services.
- Chang MH (2007) Hepatitis B virus infection. Semin Fetal Neonatal Med 12: 160-1676.
- Hou J, Liu Z, Gu F (2005) Epidermology and prevention of hepatitis B virus Int J Med Sci 2: 50-67.
- Centers for Disease Control (2016). Hepatitis B: general information.
- National Population Commission (NPC) (2008). Federal Republic of Final 2006 census results.
- Simmons (1997). Practice of Haematology. In: Technical haematology. 3rd Edition, J.B. Lippincolt Company. Philadelphia 105-116.
- Cheesbrough M (2006) Heamatological tests in District Laboratory Practice for Tropical Countries Part (2).Low Price edition United Kingdom: Cambridge university press 226-329.
- Musa BM, Bussell S, Borodo MM, Samaila AA, Femi OL (2015) Prevalence of hepatitis B virus infection in Nigeria, 2000-2013: A systematic review and meta-analysis. Niger J Clin Pract 18: 163-172.
- Jeremiah ZA, Tony-Enwin EO (2009) Seroepidemiology of Transfusion Transmissible Viral Infection among University Fresh Students in Port Harcourt, Hepatitis Monthly 9: 276-281.
- Onwuasoanya UF, Ihongbe JC, Obeagu EI, Ifeanyichukwu MO, Nwachukwu PE, et al. (2017) Evaluation of Some Immunological and Haematological Indices of Hepatitis B Infected Subjects in Nnamdi Azikiwe University Teaching Hospital, Nnewi, Anambra State, Nigeria. Journal of Biomedical Sciences 6:
- Poulsen OM, Breum NO, Ebbehoj N, Hansen AM, Ivens UI, et al (2010) Haematological Assessment of Hepatitis B Infected Patients. Journal of Applied Sciences. 7: 3562-3566.
- Goldsby G, Kindt B, Obsorne N (2007) Kuby Immunology. 6th edition. W.H. Freeman Company 574.
- Azuonwu O, Frank-Peterside N, Ibe SN, Erhabor O (2012) Risk factors associated with incidence of HIV/AIDS and HBsAg co-infection in Niger Delta Communities of Journal of Applied Pharmaceutical Science. 2: 85-91.
- Obire O, Nwankwo UJ, Ramesh RP (2009) Incidence of HIV and AIDS in Ahoada, Port Harcourt, Nigeria. Electronic Journal of Biology 5: 28-33.
Citation: Azuonwu O, Frank-Peterside N, Azuonwu TC (2020) Investigation of the Impact and Spatial Hematological Variations among Subjects infected with Hepatitis B Virus in some Niger Delta Communities. J Hematol Hemother 5: 009.
Copyright: © 2020 Azuonwu O, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and re- production in any medium, provided the original author and source are credited.