*Corresponding Author:
Itoua Okouango YS,
Multidisciplinary Research Team in Food and Nutrition (Eprancongo), Laboratory of Nutrition and Human Nutrition BP: 69, Fac- ulty of Science and Technology, Marien NGOUABI University, Department of Masters, Course: Biological Sciences Brazzaville, Congo
E-mail: yvonvasther@gmail.com
Abstract
In Congo Brazzaville, the prevalence and causes of obesity are less well-known, let alone in schools, despite the efforts of the scientific community in the epidemiological, pathophysiological and genetic fields. The objective of our survey was to highlight by-excess malnutrition in children schooled in colleges of Brazzaville while determining their prevalence of overweight and obesity as well. We achieved an anthropometric measures and transverse investigation among 825 pupils.
The results show that the global prevalence of overweight (included obesity) among the pupils is of 3.7% with respective prevalence of overweight and obesity of 3 % and 0.7 %.
With regard to the professional sectors of the heads of families, the results show that 61.5 % of pupils’ heads of households are civil servants, 26 % of their heads of families work in private sector, 3.5% of pupils have workers as heads of families and 9. 1 % of pupils’ heads of families are in informal sector. Concerning the food behavior, the results show that 83.6 % of pupils take dinner while 6.1 % never take it. As far as physical activities are concerned, the results show that 63.3 % of pupils on the whole don’t practice any extra-curricular physical activity and 75.0 % of pupils on the whole of which 59.3 % for the private junior high schools and 89.4 % for the public junior high schools go to school on foot.
In the light of this survey, we can say that a problem of overweight and obesity really exists in Congo.
Keywords
Infantile; Obesity; Overweight
Introduction
Overweight and obesity are a major public health problem world- wide because of their potential health impact and increasing frequency. The prevalence of childhood overweight and obesity has been increasing rapidly in most industrialized countries in recent years and is also expanding in countries with transition economies [1-5]. Obesity in children is also a significant risk of persistence in adulthood. It is characterized by the accumulation of excess body fat and can be conceptualized as the physical manifestation of a chronic energy surplus [6].
Long regarded as a simple aesthetic problem related to the sin of greed, obesity is today recognized as a real pathology to the point that WHO declares it as “the first non-infectious epidemic of history and a major problem of century “. Its evolution is very worrying because the number of obese adults is increasing in developed countries; but it also increases alarmingly in developing countries among which, one could mention, Congo-Brazzaville [7-10]. Obesity is increasingly affecting young people; that childhood and juvenile obesity, formerly marginal, is commonplace in the most industrialized countries such as the United States, and its incidence in developing countries continues to grow.
Many recent studies have indicated that the prevalence of adolescent obesity has increased worldwide [11-13]. For this purpose, a study done on adolescents in Tunisia by [14,15], indicates that 6.7% of students are overweight and obese.
A cross-sectional study conducted by WHO (2003) on the prevalence of overweight and obesity among junior and high school students found that 62% of regions in the Americas were overweight and 26% were obese. In Southeast Asia, the results gave 14% excess weight in both sexes, 3% for obesity. However, obesity that appeared during childhood and adolescence leads to an excess mortality in adulthood estimated at between 50 and 80% because of the associated complications (dyslipidemia, insulin resistance, chronic inflammatory state, cardiovascular diseases, metabolic diseases, respiratory diseases and some forms of cancer), also early mortality [16-22].
The causes of childhood obesity are relatively well identified, particularly in developed countries, but are much less so in developing countries. It is therefore important to know the prevalence of obesity, and to better understand the causes and mechanisms of these complications in order to better prevent this pathology for the populations concerned.
In Congo Brazzaville, the prevalence and causes of obesity are less well-known, let alone in schools, despite the efforts of the scientific community in the epidemiological, pathophysiological and genetic fields. Thus, our study is part of the knowledge of the prevalence of overweight and obesity among adolescents in the colleges of Brazzaville and the related causes.
The general objective of our work is to determine the prevalence of overweight and obesity among adolescents attending colleges in Brazzaville.
Materials and Methods
Equipment Target population
Students, attending public and private high schools in Brazzaville, capital of the Republic Congo, was chosen as the study population.
Anthropometric material
This material consisted of: a scale (that allowed us) to weigh the pupils and measure their weight; a tape measure ( used)to measure the abdominal perimeter of students and a board that allowed us to measure the size of students.
Teaching materials
The didactic material consisted of a survey sheet that was used to collect data from students. It includes the following parts: identification of the student, anthropometric measurements of students, general information about students, information about the students’ parents, perception of students’ nutrition, practice of physical activities and how students go to school.
Methods
Type of survey and study of variables
This is a cross-sectional survey of a sample of junior high school students in Brazzaville with nutritional variables (qualitative and quantitative) and with anthropometric measurements which consist of collecting data on overweight and obesity.
Sampling and survey method
To determine the sample, we proceeded by a random draw with regard to the schools. Four establishments were selected in Bacongo and Djiri districts, which were chosen in a reasoned manner. The institutions that were the subject of our study are private and public junior high schools, ranging from sixth to third grade.
Our sample is 825 students in the four schools. The choice of students in the schools was made in a comprehensive manner for each classroom.
The field work consisted
Interviewing the students, using a questionnaire established on a survey sheet, including: the identification of the student, the most often consumed type of food, the frequency of consumption, anthropometric measurements of students; information on parents of pupils; physical activity; movement of students for school.
Choice of the indicator
For this study, we used the WHO references to estimate the frequencies of overweight and obesity.
Inclusion criteria
The inclusion criteria for this study are:
- Agreeing to participate in the survey
- Residing in the city of Brazzaville at the time of the investigation;
- Attending general education junior high schools at the time of the survey;
- Accepting anthropometric
Study Site, Field Work and Collected Data
This study took place in Brazzaville junior high schools (general education), for one month (January to February 2019). The work consisted of a food and nutrition survey with anthropometric measurement. The data was collected by individual questionnaires. The collected information was based on the socio-economic data of the household, the child’s diet, and the anthropometric parameters.
Data processing
The data analysis was done thanks to the creation of a database in the software Epi-info6, Word and Excel. The student or comparison test was used. It makes it possible to decide whether the difference observed between the two movements is attributable to a systematic cause or whether it can be considered as the effect of a fluctuation due to chance.
Results and Discussion
Results
Gender, age and body mass index of students
Table 1 presents the gender, age and body mass index of students.
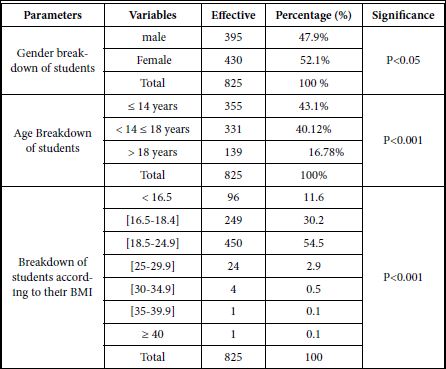
Table 1: Distribution of students by location, dwelling characteristics and professional sector of head of household.
The results in this table reveal that there are more female students (52.1%) than men (47.9%). Overall, the difference is very significant because p<0.001.
The age ranges from 11 to 20 years old and up. The most represented respondents, as a whole, are those aged between 11 and 14 (years) (43.1%); followed by those aged from 15 to 18 years of age (40.12%). Individuals whose age is greater than 20 years are the least represented (16.78%), with p>0.05.
Regarding the body mass index (BMI), 3.0% of students have a BMI between 25 and 29.9 kg/m², which is overweight and 0.7% have a BMI of 30 to more than 40 kg/m², which corresponds to obesity. These are as follows: 0.5% for type I obesity (30-34.9 kg/m2); 0.1% for type II obesity (35-39.9 kg/m2); and 0.1% for type III obesity (40 kg/m² and above). The percentage of underweight is 11.6%; 30.2% of students are skinny and 54.5% are of normal body size. The difference is very significant overall because p<0.001.
Sociodemographic characteristics
Table 2 presents sociodemographic characteristics. The results in Table 2 show that 86.3% of students live with their parents, and 13.7% live elsewhere (aunts, uncles, grandparent’s...), whose difference is not significant p>0.05.
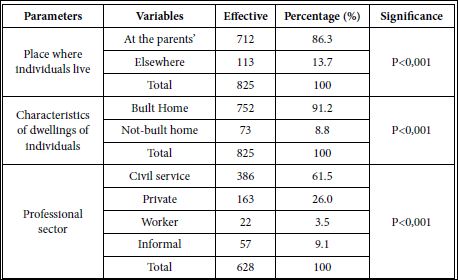
Table 2: Distribution of students by location, dwelling characteristics and professional sector of head of household.
With regard to the Characterization of student housing, 91.2% of students live good homes compared to 8.8% of students who in poor quality homes, of which P>0.05.
With regard to the professional sector of heads of households, the results show that 61.5% of the surveyed students have heads of families who are civil servants, 26.0% of students have heads of families who work in the private sector, 3.5% of students have workers as heads of families and 9.1% of students have heads of families working in informal sector, p<0.001.
Frequency of taking meals
Table 3 presents the distribution frequency, the place where breakfast is taken and people with whom students eat breakfast, and the food consumed.
The results obtained in this table show that the majority of students, 86.1%, almost take breakfast every day; 6.8% take it 3 to 5 times a week; 1.2% of students take it once or twice a week and 5.9% never take it, with p<0.001.
Place of taking meals
From Table 3, it appears that the majority of students, 82.6%, have breakfast at home; 17.1% take it at school; 0.1% of students eat it in restaurants; and 0.1% take it elsewhere (in friends’, ...), with p<0.001.
With regard to the people with whom the Breakfast is shared, more than half of the surveyed students (54.3%) have breakfast with their families; 29.0% take it alone. It also shows that 16.6% take it with friends; and 0.1% take it with other people (either at the restaurant or in other households). Overall, the difference is very significant (p<0.001).
Type of food eaten, most often, as breakfast: the results show that 60.7% of students have as breakfast Milk+spread bread; 34.1% of students take other food (grills ...). Students who take juice+plain or spread bread (4.4%); milk+flour donut (0.5%). And, those who take milk + plain bread (0.3%) are poorly represented, p<0.001.
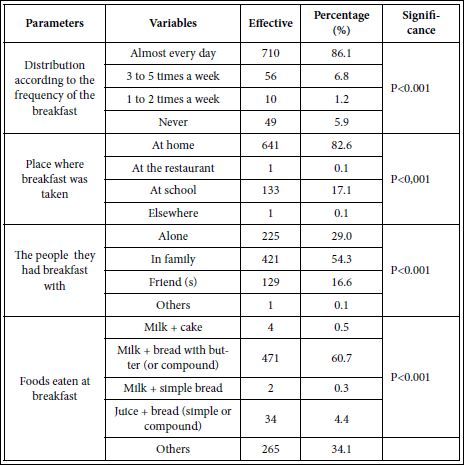
Table 3: Distribution of frequency, place of breakfast, persons with whom they eat breakfast and consumed food.
Lunch
Table 4 shows the distribution frequency, the place where breakfast is taken, people they have lunch with, and the consumed food.

Table 4: Distribution frequency, place of lunch, persons with whom they take lunch and food consumed.
It shows that 86.5% of students almost take breakfast every day; 3.8% have lunch 3 to 5 times a week; 0.7% have lunch 1 to 2 times a week and 9% do not take it. The difference is not significant (p>0.05).
Regarding the place where the lunch was consumed: the results show that 88.7% of students take lunch at home; 11.2% take it at the canteen (at school); and, 0.1% takes it elsewhere (garrotes’ ...), p<0.001.
Most students (69.2%) have lunch with their families; 19.7% take it alone; 10.9% of students take it with friends and 0.1% take it with other people (at the restaurant, in other households, ...). with p<0.001.
Regarding eating habits, it also appears that at lunch, students consuming frozen products are the most represented (65.1%). Then come those who consume freshwater fish (smoked or salted) (21.0%); and 13.7% of those who take other food (porridge ...). Students taking plain or spread bread (0.1%) are poorly represented, p>0.05.
Having dinner
Table 5 presents the distribution frequency, the place where dinner is taken, the people with whom they take dinner, and the food consumed.

Table 5: Distribution of frequency, place where dinner was taken, people they take dinner with and food consumed.
With regard to dining, these results show that 83.6% of students take dinner every day or almost every day; 6.4% take it 3 to 5 times a week; 3.9% take it once or twice a week; finally 6.1% never take it, whose difference is not significant (p>0.05).
Regarding the place of dinner consumption, the results show that 99.9% of students take it at home and 0.1% take it elsewhere (restaurant, other households, ...), with p<0.001.
Most students (79.6%) are as follows, 74.9% take their dinner with their family compared to 20.4% who take it alone (p<0.001).
Regarding eating habits, 0.3% of students at dinner consume bread (plain or spread), 29.3% consume frozen food (more accompaniment). 20.9% of students consume other foods than those mentioned before and 7.0% consume freshwater fish (smoked, salted, plus accompaniment); and 42.6% consume bread+milk, p<0.001.
Nibbling
Table 6 presents the snacking frequency, the snacking reasons and the category of food nibbled by the students.
The results in this table show that the majority of students (71.9%) nibble between meals against 28.1% who do not nibble, p>0.05.
It also appears that most students nibble routinely (59.7%) when others (43.3%) nibble because they are hungry, the difference is very significant (p<0.001).
These results clearly show that sweet foods (sweet biscuits, ice cream...) are the most consumed during snacking (85.8%); followed by salty foods (sausages, chips ...) with a percentage of 13.7%. The category of foods the least consumed is that of dairy products (yogurt, cheese,) with a percentage of 0.5%, with p<0.001.
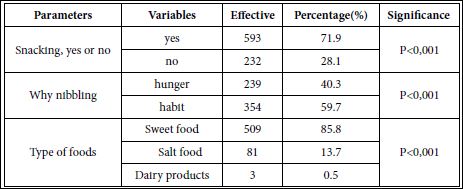
Table 6: Distribution according to whether students are snacking or not, why nibbling and the category of food nibbled.
Physical activity and type of transportation
Table 7 presents the distribution of students according to the types of sport they practice or not, and according to students means of moving to school.
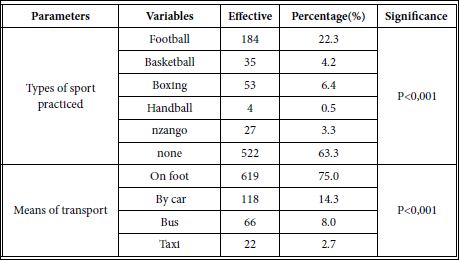
Table 7: Distribution of students by type of sports they practice or not and by means students go to school.
a) Type of sport
It can be seen from this table that the majority of students (63.3%) do not practice any extracurricular physical activity, only 36.7% practice sport among them those who practice football are 22.3%. Students practicing boxing, 6.4%; basketball, 4.2%; “nzango”(sport practiced by women using only their feet), 3.3%; handball, 0.5 % (p<0.001).
b) Means of transport
The analysis of these results shows that 75.0% of students go to school on foot. It follows 14.3% who go by car (personal); 8.0% of students go by bus. Finally, 2.7% go by taxi (p<0.001).
Discussion
Our study aims to assess the prevalence of overweight and obesity among children attending junior high schools in Brazzaville; and to identify the factors influencing the development of this weight gaining. The overall rates obtained in our study on the prevalence of over- weight and obesity are respectively 3% and 0.7% in a sample of 825 students. This study indicates the existence of overweight problems among students in Brazzaville. In South Africa, [23] indicate 4% over- weight among 8-11 year old schoolchildren. The prevalence of over- weight in our study (3%) is close to that obtained by [4] in Togo on 1224 students in junior high schools with an overweight prevalence of 2.8% and obesity of 1.72% . The overall prevalences we found differ from those reported in Ivory Coast, by [22], with a prevalence of obesity of 5% while overweight affects 4% of children.
Concerning the professional sector of the household head
The majority of them are civil servants (61.5%); 26% are employed in the private sector; 3.5% are manual workers and 9.1% are in the informal sector. These values differ from those reported by SEMEP (2011) in Algeria [24], with 29.5% of employees and 7.9% of workers. They also differ from those obtained by [14], in Tunisia of whom 58.9% are workers, 22.5% employees and 3.6% informal.
With regard to eating habits
Our study shows that, on the whole, the majority of children (85.4%) on average usually eat the main meals of the day (breakfast, lunch, dinner); that is 86, 1% of children who eat breakfast; 86.5% have lunch; and 83.6% have dinner. It also indicates that most children eat at home, 90.4% on average; and in most cases for families, 67.7% on average. These results are similar in terms of frequencies and location of meal consumption to those obtained in Algeria by SEMEP (2011) which found respectively 80% of children who usually took their main meals; 94% who took them home; as well as those reported by [14] in Tunisia with 87.7% of children who usually took the main meals, 97.4% took them home. But they differ with regard to people with whom they share meals (82%) for SEMEP and 85.2% for [14].
Our study also shows that 5.9% of students never eat breakfast, 9.0% do not eat breakfast, and 6.1% do not eat dinner. These results differ from those obtained by [14], in Tunisia, who found 24% of students who did not have breakfast; 2.7% who did not have lunch; and 9.9% who did not take dinner.
Regarding the feeding practices, the results obtained indicate, at breakfast, that more than half of the children (60.7%) take milk + spread bread (butter, chocolate, ...) and 34.1% take other things ( spaghetti, rice, ...); at lunch, 65.1% of the children take imported meats (chicken, chicken leg, ...) plus accompaniment (cassava, bread, rice and others) and barely 21.0% take fresh fish; at dinner, 42.6% of children take milk + bread (simple or spread) and 29.3% eat imported meat (chicken, chicken leg, ...) plus an accompaniment (cassava, bread, rice and others). The meals taken by the students in our study are generally characterized by a fat diet, which is a major factor in the weight increase.
Our study shows that 71.9% of students nibble between meals of whom 85.8% munch on sweets; 13.5%, salty; and 0.5%, dairy products. SEMEP (2011), in Algeria, found that 60% of students took sweets, 78% took imported meats and 48% took fish. But the category of food, the most consumed by these students, promote a dietary imbalance, and the least consumed food, as fish, is essential to the nutritional balance and needs of children and adolescents (SEMEP, 2011). This poor eating behavior is among the causes of overweight observed in children and adolescents.
Also, the destructuring of meals (breakfast jump and important calorie intake in the evening) promotes weight gain. It is important to note that a high sugar intake is associated with less satiety, which does not favor the reduction of ingested doses.
With respect to physical activity practice and how students leave to school, these results show that most of these students (63.3%), overall, do not engage in physical activity except during physical education (PE) at school, and 36.7% on average practice it; 75% of students go to school on foot, 17% on average go by car(personal car and taxi) and 8% go by bus. Our results are close to those indicated by the SEMEP (2011), in Algeria ,which found 34% of children who practiced an extracurricular sporting activity, 74% who went to school on foot, 18% went there by car and 8 % by bus. These sedentary lifestyles or inactive behaviors promote food intake and obesity in children and adolescents [25].
Conclusion
The results obtained from this study, on the one hand, allowed us to have an overview of the prevalence of overweight and obesity in schools in Congo Brazzaville. On the other hand, they allowed us to have an idea about the different factors influencing this weight gain in students, the professional status of the head of the family associ- ated with the decrease of the practice of physical activity. Brazzaville junior high school students are adopting a way of life that can trigger a problem of overweight in the future. In the end, overweight chil- dren should be closely monitored and all ways to lose weight should be considered.
References
- Oulamara H, Agli AN, Frelut ML (2006) Alimentation, activité physique et surpoids chez des enfants de l’Est Algérien. Cah Nutr Diét 41: 46-54.
- Taleb S, Agli AN (2009) Obésité de l’enfant: rôle des facteurs socioéconomiques, obésité parentale, comportement alimentaire et activité physique, chez des enfants scolarisés dans une ville de l’Est algérien. Cah Nutr Diét 44: 198-206.
- Jacobi D, Buzelé R, Couet C (2010) Peut-on parler de pandémie d’obésité ? Presse Med 39: 902-906.
- Djadou KE, Sadzo-Hetsu K, Koffi KS (2010) Prévalence de l’obésité en milieu scolaire urbain (Togo). Journal de pédiatrie et de puériculture 23: 335-339.
- Bulbul T, Hoque M (2014) Prevalence of childhood obesity and overweight in Bangladesh: Findings from a countrywide epidemiological study. BMC Pediatrics 14: 86.
- Chaput JP, Tremblay A (2012) L’obésité précoce et ses impacts sur le développement de l’enfant. Encyclopedie sur le developpement du jeune enfant 20: 1-8.
- Ezzati M, Lopez AD, Rodgers A, Vander HS, Murray CJ (2002) Comparative Risk Assessment Collaborating Group. Selected major risk factors and global and regional burden of disease. Lancet 360: 1347-1360.
- Sibai AM, Hwalla N, Adra N, Rahal B (2003) Prevalence and covariates of obesity in Lebanon: Findings from the first epidemiological Obes Res 11:1353-1361.
- Stevens J, Murray DM, Baggett CD, Elder JP, Lohman TG (2007) Objectively assessed associations between physical activity and body composition in middle-school girls: The Trial of Activity for Adolescent Girls. Am J Epidemiol 166: 1298-1305.
- James Y, Steinberg JG, Brégeon F, Delliaux S (2004) The oxidative stress in response to routine incremental cycling exercise in healthy sedentary subjects. Respir Physiol 144: 81-90.
- Haslam DW, James WP (2005) Lancet 366: 1197-1209.
- Hanley AJ, Harris SB, Salsvig B, Zinmar B (2000) Overweight among Children and adolescents in a native Canadian Community: Prevalence and Assocated Factors. Am.J Clin Nutr 71: 693-700.
- Oduwole AA, Ladapao TA, Fajolu IB, Ekure EN, Adeniyi OF (2012) Obesity and Elevated Blood Pressure among Adolescents in Lagos, Nigeria : A cross-sectional study. BMC Public Health 12 : 616.
- Zedini C, Limam M, Ghardallou ME, Mellouli M, Sahouda K (2016) Prévalence de la surcharge pondérale en milieu La tunisie Medicale 94: 304-398.
- OMS (2003) Obésité: Prévention et prise en charge de l’épidémie mondiale. Série de rapports techniques. Genève: OMS 894: 300.
- Kopp P, Kopp CW, Festa A, Krzyzanowska K, Kriwanek S (2003) Impact of weight loss on inflammatory proteins and their association with the insulin resistance syndrome in morbidly obese patients. Ar- terioscler Thromb Vasc Biol 23: 1042-1047.
- Biro FM, Khoury P, Morrison JA (2006) Influence of obesity on tim- ing of puberty. Int J Androl 29: 272-277.
- Herder C, Hauner H, Haastert B, Rohrig K, Koenig W (2006) Hy- poadiponectinemia and proinflammatory state: Two sides of the same coin? Results from the Cooperative Health Research in the Region of Augsburg Survey 4 (KORA S4). Diabetes Care 29: 1626-
- Stevens J, Murray DM, Baggett CD, Elder JP, Lohman TG (2007) Objectively assessed associations between physical activity and body composition in middle-school girls: The Trial of Activity for Ad- olescent Girls. Am J Epidemiol 166: 1298-3105.
- Taleb S, Agli AN (2009) Obésité de l’enfant: rôle des facteurs so- cioéconomiques, obésité parentale, comportement alimentaire et activité physique, chez des enfants scolarisés dans une ville de l’Est algérien. Cah Nutr Diét 44: 198-206.
- Mabiala Babela JR, Sabaye AJ, Monabeka HG, Mbika Cardorelle A, Nkoua JL (2011) Profil épidémiologique et clinique de l’obésité de l’enfant à Brazzaville (Congo). Cah Nutr Diét 46: 259-262.
- Kramoh KE, Ngoran Y, Aké-Traboulsi E (2012) Prévalence de l’obésité en milieu scolaire en Côte d’Ivoire. Ann Cardiol Angeiol 61: 145-149.
- Jinabhai CC, Taylor M, Sullivan KR (2003) Implications of the prev- alence of stunting, overweigt and obesity amongst South African primary school children: A possible nutritional transition. Eur j Clin Nurt 57: 358-365.
- Service d’Epidémiologie et de Médecine Préventive (2011). Etude du surpoids, de l’obésité et des facteurs associés au surpoids chez les élèves du cycle moyen scolarisés dans les collèges publics de l’Etablissement Public de Santé de Proximité
- Rennie K, Johnson L, Jebb SA (2005) Behavioural determinants of obesity. Best Practice and Research Clinical Endocrinology and Metabolism 19: 343-58.
Citation: Okouango IYS, Vital M, Michel E, Delvina ON (2020) Infantile Overweight and Obesity in School (Colleges) in Brazzaville. J Nutr Food Sci 3: 017.
Copyright: © 2020 Okouango IYS, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and re- production in any medium, provided the original author and source are credited.