*Corresponding Author:
Ariel Beresniak,
Data Mining International, Route de l’Aéroport, 29-31, CP221, CH-1215 Geneva Switzerland
Tel: + 41 227993400
Fax: + 41 227883850
E-mail: aberesniak@datamining-international.com
Abstract
Background: Facial imperfections may negatively affect the Quality of Life (QoL) of individuals with facial aesthetic imperfections. The objective of this study was to assess the impact of two cosmetic camouflage products (an opaque cover cream and a low coverage loose powder) on the QoL of women with facial aesthetic imperfections.
Methods: A randomized controlled open study was carried out on 88 women presenting facial aesthetic imperfections using either a cover cream or a loose powder during a 3 weeks period. The French version of the Beauty Qol® instrument, a QoL tool specific in cosmetic products, has been completed at D1, D7 and D21.
Results: The results of the study show that after 3 weeks of daily use, both camouflage products have improved the QoL in subjects with facial aesthetic imperfections. Results suggest that the cover cream would consistently improve QoL better than the loose powder, with significant statistical differences for the dimension “Self confidence” at day 7.
Conclusions: This study demonstrates that camouflage products contribute to improving the QoL of individuals presenting facial aesthetic imperfections. Given its specificity in cosmetology, the Beauty QoL® instrument will enable further research on QoL across a wide range of skin pigmentary disorders.
Introduction
Skin is the most important component of an individual’s physical appearance; cosmetic defects do greatly interfere with social life, work and relationships [1-3]. Facial appearance also plays a large role in self-perception and interaction with others [4-6].
Although facial aesthetic imperfections may be perceived as common and trivial, they impair quality of life (QoL) [7]. Visible skin lesions and pigmentary disorders have been reported to negatively impact self-image, self-esteem, and different dimensions of the Quality of Life, and cause a significant burden and psychological distress [1,816]. People with visible facial defects are repeatedly stared at, or even avoided. In some cultures, a different skin appearance may also lead to social stigmatization [3,17].
Broadly QoL infers an individual’s total well-being [18]. This multidimensional concept and its determinants have evolved to represent physical or mental Health-Related Quality of Life (HRQoL) [19,20]. It now includes all emotional, social and physical aspects of the individual’s life, and how they may be impacted over time by a disease, a disability or a disorder. Consequently, and to the extent that cosmetics help improve our appearance, they can affect how we relate to ourselves and to others, and as such, can improve well-being [21].
There is a growing field of research concerned with developing, assessing, and applying QoL measures within health related research, including in cosmetology. QoL is typically assessed using self-administered multidimensional questionnaires which are either generic (general health), domain specific (e.g. dermatology) or disease-specific [22,23]. They cover physical, social, emotional, cognitive, workor role-related, and other aspects that contribute to an individual’s well-being.
While many skin conditions are amenable to treatment, on certain occasions, cosmetic camouflage can also alleviate the suffering of those who have been disfigured by a scar or by a congenital or other acquired lesions [24-26]. The use of decorative cosmetics is thus an effective and well-tolerated measure which has been shown to significantly improve the appearance and the QoL of individuals affected by skin disorders [5,7,14,27-32]. For instance, corrective camouflage can help cover cutaneous unaesthetic disorders using a variety of water-resistant, and light to opaque products that provide effective and natural coverage. These products also can serve as concealers and nicely complement potential medical treatments, or follow the surgical procedures before healing is complete [33,34]. Cosmetic camouflage techniques can significantly improve QoL in subjects with apparent skin disorders [28,29]. A good cover cosmetic should have the following characteristics: opaque, greaseless, waterproof, easy to apply, long-lasting, fragrance-free, non-irritating, non-sensitizing, non-photosensitizing and non-comedogenic, be applicable to all skin types, and yet “look natural”. Camouflage makeup products contain agents that provide coverage (e.g. iron oxide pigment, titanium dioxide, kaolin). Because of our ethnic differences they need to provide in many different shades [24] and come in a variety of finishes: matte, semimatte, moist semimatte, and shiny. The foundations come in a variety of forms, liquids, mousse, water-based cream, loose powder, stick, and lotions [26]. Considering that some skin lesions may demonstrate subtle textural and pigment changes, while others may be more complex, the camouflage techniques and products should be adapted to the skin disorder. For mild problems, a simple foundation product usually suffices (with or without a colour corrector). But for more apparent facial aesthetic imperfections, full concealment creams might be needed. However, mixing products and formulations (e.g. foundations, concealers, powders and blushers) in different parts of the face may help achieve the desired look and the appropriate level of coverage [24].
Albeit the relationships between physical attractiveness, cosmetic practices and self-perception have been studied [35], few data exist on the positive effects of non-surgical cosmetic measures on QoL [36]. Their potential benefits may now be objectively established using validated methods and QoL instruments. In the last two decades, a number of instruments have been developed to assess the effects of different conditions and therapeutic measures on perceptions of well-being, and the value that individuals place on their dermatology state of health [37]. With the recent development and the international validation of the BeautyQoL® specific questionnaire [38], it is now possible to assess and demonstrate scientifically how cosmetic products impact QoL in subjects with skin pigmentary disorders. The objective of this study was to assess the impact of two cosmetic camouflage products (a cover cream and a loose powder) on the QoL of women with facial aesthetic imperfections.
Methods
A randomized, monocentric, open study has been conducted in France involving 88 healthy volunteer women (18-45 years old) with facial aesthetic imperfections. All subjects were females between 18 and 45 years old having aesthetic imperfections (scars from acne, chickenpox or pigmentary disorders such as melasma). Subjects were selected based on a recruitment questionnaire and a thorough clinical examination performed by the clinical investigator according to inclusion and exclusion criteria (Table 1).
Table 1: Inclusion and Exclusion Criteria.
The subjects were randomized to the daily use for 3 weeks, of one of two cosmetic camouflage products, namely Product A, an opaque cover cream or Product B, a low coverage loose powder. Product A (cream) was provided in a pencil, and Product B (powder) in a compact. Each subject was followed during a period of 3 consecutive weeks, over a total of 3 visits: one visit at study enrolment (Day 1), one follow up visit (Day 7), and one final visit at the end of the study period (Day 21). During the last 2 visits, the subjects had to come with their makeup on. The study was performed in compliance with the recommendations from the World Medical Association (Declaration of Helsinki in 1964, amended in 1975, 1983, 1989, 1996 and 2000), and in compliance with general principles of the Good Clinical Practice guidelines ICH Topic E6 (May 1996). All subjects enrolled in the study provided their signed informed consent. The French version of the BeautyQoL® instrument [38] was used to assess the potential improvement on QoL dimensions of the cosmetic camouflage products being studied. The BeautyQoL® questionnaire consisted of 42 items assessing five QoL dimensions: social life, self-confidence, mood, energy and attractiveness.
Demographics data were collected, including the skin phototype according to the Fitzpatrick skin-type score [39]. At Day 1, the BeautyQoL® questionnaire was self-administered, followed by a clin- ical questionnaire relevant to the facial aesthetic imperfections, and a general health questionnaire. The BeautyQoL® questionnaire was also self-administered at Day 7 and Day 21.
A professional makeup trainer, under the responsibility of the investigator, informed each subject of the colour determined by the phototype. She indicated to each subject the recommended application for the study product supplied: once daily, preferably in the morning, during the 3 weeks of the study. The subject had to continue her daily routine (hydration and makeup), including the use of her regular foundation. The subject had to remove the makeup in the evening with the cleanser provided for the study.
Results
Mean age was 30 from a minimum of 18 and a maximum of 45 (Table 2). At enrolment, fourteen subjects had at least one medical history, and five had a concomitant treatment. However, the medical examination confirmed the status of healthy volunteer for all the study subjects. Two subjects withdrew prematurely from the study for personal non medical reasons.

Table 2: Demographic data.
The 86 remaining subjects have all met the requirement of the study protocol, and proper use of the products being studied. No protocol deviation was observed. The results related to the QoL obtained from the BeautyQoL® questionnaire on Day 1 (study enrolment) confirm the homogeneity of the groups according to QoL (global score 52,9 for group A versus 51.9 for group B). At Day 7 and Day 21, the results confirm that both Product A (cream) and B (loose powder) improved the QoL of subjects. At Day 7, QoL scores appear higher for product A than for product B in all dimensions: 46.3 versus 43.3 for “Social Life”, 58.3 versus 51.6 for “Self confidence”, 51 versus 45.3 for “Mood”, 43.2 ver- sus 43.02 for “Energy”, 47.9 versus 44.2 for “Attractiveness” and 49.7 versus 45.2 for “Global score” (Figure 1). At Day 21, QoL scores again appear higher for product A than for product B in all dimensions: 49.2 versus 46.5 for “Social Life”, 59.3 versus 54.8 for “Self confidence”, 52.8 versus 48.2 for “Mood”, 48.4 versus 45.4 for “Energy”, 52 versus 47.5 for “Attractiveness” and 52.5 versus 48.6 for “Global score” (Figure 2). Wilcoxon tests established that these differences were not statistically significant, excepting at Day 7 for the dimension “Self Confidence (p<0.05).

Figure 1: Group A Beauty Qol® scores at Day 0, Day 7 and Day 21.
Discussion
Because of the very recent use of Quality of Life instruments to assess cosmetic disorders, no studies have yet been published comparing the impact on QoL of two camouflage products, confirming the interest of this study. The results show that after 3 weeks of daily use, two cosmetic camouflage products, namely an opaque cover cream and a low coverage loose powder, were well tolerated and contributed to improving the QoL in healthy female volunteers with facial aesthetic imperfections, as confirmed by favourable BeautyQoL® scores relevant to the different QoL dimensions: social life, self-confidence, mood, energy and attractiveness. When considering all scores across QoL dimensions, and although not always significantly different, the results suggest that the cover cream had performed better than the loose powder. The main limitation of this pilot study however remains the arbitrary number of subjects, which have been defined without statistical assumptions. This is the case of most of exploratory studies involving a new tool in a new context, and suggests that further research in a broader population, including for different types of facial pigmentary disorders, would contribute to strengthening the generalization of the results. Thus, the lack of significant statistical differences is probably due to a low number of subjects. However, this study provides the necessary distribution assumptions to be able to calculate the sample size of further comparative studies.
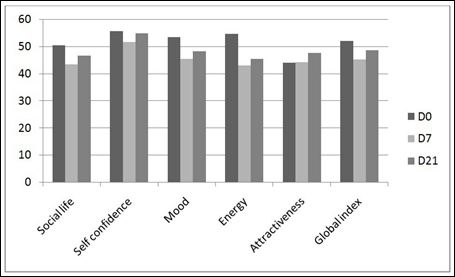
Figure 2: Group B Beauty Qol® scores at Day 0, Day 7 and Day 21.
Another limitation of this study, which is shared with most of comparative clinical trials, is that there is no specific arm assessing a combination of the two products, cream topped up with a camouflage powder, which is known to give better results than products used individually. This combination is widely used in practice and promoted by many cosmetic companies. However, interpretating the outcomes of a combination are much more difficult than comparing single products in the frame of a clinical study.
The selection of the BeautyQoL® questionnaire as QOL outcome has been supported by the very good psychometric properties, such as high internal consistency, reproducibility, and reliability, as well as significant correlation with the Short Form Health Questionnaire (SF36) [38], which supports the robustness of the results.
This original study conducted in France on 88 healthy females with facial aesthetic imperfections establishes that two cosmetic camouflage products can restore physical appearance to a cosmetically acceptable level, and improve at the same time all dimensions of QoL. Considering that many pigmentary disorders are known to have a deleterious effect on QoL, the findings of this pilot study suggest that more research using validated QoL instruments is needed to firmly establish the benefits of cosmetic products on improving QoL in a broad range of pigmentary disorders.
Declaration of interest
Yolaine de Linares is employee of L’Oréal Research and Innovation.
References
- Taylor A, Pawaskar M, Taylor SL, Balkrishnan R, Feldman SR (2008) Prevalence of pigmentary disorders and their impact on quality of life: a prospec- tive cohort J Cosmet Dermatol 7: 164-168.
- Basra MK, Shahrukh M (2009) Burden of skin Expert Rev Pharmacoecon Outcomes Res 9: 271-283.
- Schmid-Ott G, Steen T (2010) Skin Disorders and Quality of In Stone JH, Blouin M (eds.). International Encyclopedia of Rehabilitation.
- Balkrishnan R, McMichael AJ, Hu JY, Camacho FT, Shew KR, et al. (2006) Correlates of health-related quality of life in women with severe facial blem- Int J Dermatol 45: 111-115.
- Boehncke WH, Ochsendorf F, Paeslack I, Kaufmann R, Zollner TM (2002) Decorative cosmetics improve the quality of life in patients with disfiguring skin Eur J Dermatol 12: 577-580.
- Brown MM, Chamlin SL, Smidt AC (2013) Quality of life in pediatric dermatology. Dermatol Clin 31: 211-221.
- Peuvrel L, Quéreux G, Brocard A, Saint-Jean M, Vallet C, et (2012) Evaluation of quality of life after a medical corrective make-up lesson in patients with various dermatoses. Dermatology 224: 374-380.
- Ghajarzadeh M, Ghiasi M, Kheirkhah S (2012) Associations between skin diseases and quality of life: a comparison of psoriasis, vitiligo, and alopecia Acta Med Iran 50: 511-515.
- Segot-Chicq E, Compan-Zaouati D, Wolkenstein P, Consoli S, Rodary C, et (2007) Development and validation of a questionnaire to evaluate how a cosmetic product for oily skin is able to improve well-being in women. . J Eur Acad Dermatol Venereol 21: 1181-1186.
- Grimes PE (2009) Management of hyperpigmentation in darker racial ethnic groups. Semin Cutan Med Surg 28: 77-85.
- Hale ED, Treharne GJ, Norton Y, Lyons AC, Douglas KM, et al. (2006) ‘Concealing the evidence’: the importance of appearance concerns for patients with systemic lupus Lupus 15: 532-540.
- McElhone K, Abbott J, Teh LS (2006) A review of health related quality of life in systemic lupus erythematosus. Lupus 15: 633-643.
- Miniszewska J, Juczyński Z, Ograczyk A, Zalewska A (2013) Health-related Quality of Life in Psoriasis: Important Role of Personal Resources. Acta Derm Venereol 93: 551-556.
- Scherdin U, Bürger A, Bielfeldt S, Filbry A, Weber T, (2008) Skin-lightening effects of a new face care product in patients with melasma. J Cosmet Dermatol 7: 68-75.
- Silverberg JI, Silverberg NB (2013) Association between vitiligo extent and distribution and quality-of-life impairment. JAMA Dermatol 149: 159-164.
- Tang MM, Chang CC, Chan LC, Heng A (2013) Quality of life and cost of illness in patients with psoriasis in Malaysia: a Multicenter Study. Int J Dermatol 52: 314-322.
- Parsad D, Kumarasinge SPW (2006) Psycho-social implications of pigmentary disorders in PASPCR Commentary 1: 1-8.
- [No authors listed] (1998) The World Health Organization Quality of Life Assessment (WHOQOL): development and general psychometric properties. Soc Sci Med 46: 1569-1585.
- Gandek B, Sinclair SJ, Kosinski M, Ware JE (2004) Psychometric evaluation of the SF-36 health survey in Medicare managed care. Health Care Financ Rev 25: 5-25.
- McHorney CA (1999) Health status assessment methods for adults: past accomplishments and future Annu Rev Public Health 20: 309-335.
- Battie C, Verschoore M (2011) Dermatology, cosmetic and well-being. Ann Dermatol Venereol 138: 294-301.
- Both H, Essink-Bot ML, Busschbach J, Nijsten T (2007) Critical Review of Generic and Dermatology-Specific Health-Related Quality of Life Instru J Invest Dermatol 127: 2726-2739.
- Finlay AY (2004) Quality of life indices. Indian J Dermatol Venereol Leprol 70: 143-148.
- Antoniou C, Stefanaki C (2006) Cosmetic J Cosmet Dermatol 5: 297-301.
- Westmore MG (2001) Camouflage and makeup Clin Dermatol 19: 406-412.
- Rayner VL (2001) Camouflaging skin lesions and other disfiguring condiIn Shai A, Maibach HI, Baran R (eds.). Handbook of Cosmetic Skin Care. London, Martin Dunitz Pg no: 241-250.
- Deshayes P (2009) Cosmetic camouflage for a better quality of Ann Dermatol Venereol 135: 372-374.
- Holme SA, Beattie PE, Fleming CJ (2002) Cosmetic camouflage advice improves quality of life. Br J Dermatol 147: 946-949.
- Kent G (2002) Testing a model of disfigurement: effects of a skin camouflage service on well-being and appearance anxiety. Psychol Health 17: 377-386.
- Hayashi N, Imori M, Yanagisawa M, Seto Y, et al. (2005) Make-up improves the quality of life of acne patients without aggravating acne eruptions during Eur J Dermatol 15: 284-287.
- Kligman AM, Graham JA (1989) The psychology of appearance in the elder Clin Geriatr Med 5: 213-222.
- Tanioka M, Yamamoto Y, Kato M, Miyachi Y (2010) Camouflage for patients with vitiligo vulgaris improved their quality of life. J Cosmet Dermatol 9: 72-75.
- Tedeschi A, Dall’Oglio F, Micali G, Schwartz RA, Janniger CK (2007) Corrective camouflage in pediatric Cutis 79: 110-112.
- Titeca G, Poot F, Cassart D, Defays B, Pirard D, et al. (2007) Impact of cosmetic care on quality of life in breast cancer patients during chemotherapy and radiotherapy: an initial randomized controlled study. J Eur Acad Dermatol Venereol 21: 771-776.
- Graham JA, Kligman AM (1985) The Psychology of Cosmetic New York, Praeger publisher.
- Sadick NS (2008) The impact of cosmetic interventions on quality of life. Dermatol Online J 14: 2.
- Farage MA, Miller KW, Sherman SN, Tsevat J (2012) Assessing quality of life in older adult patients with skin Glob J Health Sci 4: 119-131.
- Beresniak A, de Linares Y, Krueger GG, Talarico S, Tsutani K, et al. (2012) Validation of a new international quality-of-life instrument specific to cosmetics and physical appearance: BeautyQoL Arch Dermatol 148: 1275-1282.
- Fitzpatrick TB (1988) The Validity and Practicality of Sun-Reactive Skin Types I Through VI. Arch Dermatol 124: 869-871.
Citation: Beresniak A, Auray JP, Duru G, Krueger GG, Talarico S, et al. (2017) Impact on the Quality of Life of Two Cosmetic Camouflage Products for Facial Aesthetic Imperfections of Skin Phototypes III and IV: Interest of the Beautyqol Instrument. J Clinic Exper Cosme Derma 1: 001.
Copyright: © 2017 Beresniak A, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
