*Corresponding Author:
Abu Khalid Muhammad Maruf Raza,
Department of Pathology, Jahurul Islam Medical College, Kishoregonj, Bangladesh
Tel: +880 1711306123
E-mail: lorenzo.alibardi@unibo.it
Abstract
Hysterectomy is the most commonly performed gynecological surgery throughout the world. Few studies have been performed describing the pathologic findings in hysterectomy specimens and examining the relationship between the preoperative clinical indication and pathologic diagnosis. This study was undertaken to identify the most common pathological lesion in hysterectomy specimens. This study was done in a medical college hospital of Bangladesh over a period of two years and two hundred and two hysterectomy specimens were included. Surgical specimens were formalin fixed and tissue was adequately processed from them. The sections were stained routinely with hematoxylin and eosin stain. Pathological findings in the uterus, cervix, ovaries and tubes were noted. Menorrhagia, fibroid uterus and uterovaginal prolapsed were the most common clinical indications for hysterectomy. The most common pathologies identified were atrophic endometrial in endometrial, leiomyoma in myometrium, chronic cervicitis in cervix, benign cystic teratoma in ovaries and salpingitis in fallopian tubes. The pathologic examination confirmed the clinical diagnosis in majority of the cases.
Keywords
Histopathology; Hysterectomy; Leiomyoma; Prolapse
Introduction
Hysterectomy, which means surgical removal of the uterus is the second most frequently performed major surgical procedure in females worldwide next to cesarean section [1]. Indications of hysterectomy vary from benign condition to malignancies of genital tract. Hysterectomy is considered definite treatment of various pelvic pathologies like leiomyoma, dysfunctional uterine bleeding, chronic pelvic pain, endometriosis, adenomyosis, prolapse and malignancies [2]. Rates of hysterectomy vary with geographic area, patient expectations and training and practice patterns of the local gynecologic surgeons. Hysterectomy can be performed by abdominal, vaginal or laparoscopic route and may or may not be accompanied by salphingo-oophorectomy of either one or both sides. However, like any other surgery, hysterectomy is also associated with intraoperative and postoperative complications [3]. We present a descriptive study where two years data of all hysterectomy cases sent for histopathology were analyzed to find out the causes for which these surgeries were performed and also to see the spectrum of histopathological changes encountered in these specimen.
Material and Methods
A descriptive study was conducted for the period of two years in the Pathology Department of Jahurul Islam Medical College and Hospital. Hysterectomy specimen sent for histopathological examination to the pathology department of Jahurul Islam medical college was included in the study. Study period was about two years from January 2015 to November 2016 and sample size was 202. The clinical history of all cases was collected from the hospital record data base. The specimens were properly labelled and kept for fixation in 10% Formalin overnight. After gross sectioning, the tissues were processed in the tissue processor and the paraffin embedded tissue blocks were cut into 5 micron thickness. After staining with hematoxylin and eosin slides were examined under microscope. Pathological findings in the uterus, cervix, ovaries and tubes were noted.
Statistical Analysis
Microsoft office 2016 software was used to generate tables. Only descriptive statistics were used to infer results.
Results
Of the 202 cases studied, the most common age group undergoing hysterectomy appeared to be 40-49 yrs (64 cases) followed by 40 (19.8%) cases in 30-39 years age group (Table 1). Mean age was found to be 40.26 years. Hysterectomy below 20 years was not found in this study and above 70 years was rare (4 cases).
The commonest complaint was per vaginal bleeding followed by feeling of fullness in the vagina and pain in the lower abdomen. Total abdominal hysterectomy with preservation of both ovaries were the most common surgical method of hysterectomy (38.6% cases) followed by vaginal hysterectomy in 25.7% cases.
Histopathological findings in the body of the uterus included leiomyoma in 60 (29.7%) cases, adenomyosis 40 (25.7%) cases, atrophic endometrial was seen in 26 (12.8%) cases, endometrial polyp in 10 (4.9%) cases and endometritis in 8 (3.9%) cases. Of the 202 hysterectomy specimen 42 (20.8%) of cases show unremarkable endometrial. Among cervical lesions, 70 (34.6%) cases showed features of chronic cervicitis followed by hyperkeratosis compatible with prolapse in 64 (31.7%) cases. Chronic cervicitis with squamous metaplasia was seen in 32 (15.8%) cases, cervical polyp in 6 (2.9%) cases, cervical dysplasia (CIN-I) and squamous cell carcinoma in 4 (1.9%) cases each (Table 2).
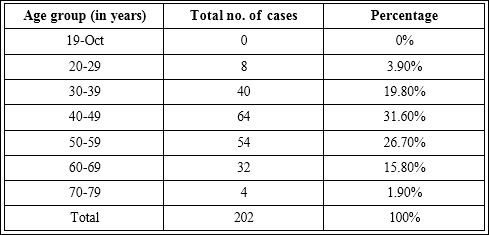
Table 1: Age wise distribution of cases (n=202).
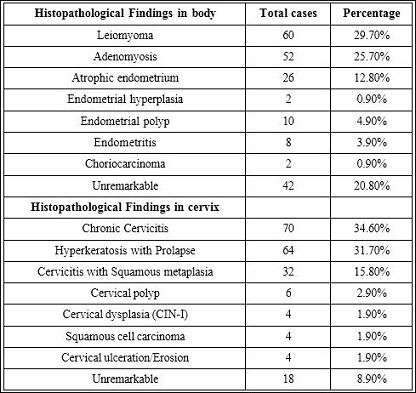
Table 2: Histopathological findings in body and cervix of the uterus (n=202).
Lesions in ovaries were benign cystic lesions including follicular cyst in 11.1% cases, serous cyst in 11.1% cases. There were serous cystadenoma and mucinous cystadenoma in 4 (5.5%) cases each. Serous cystadenocarcinoma was found in 2 (2.7%) cases. However 32 (44.4%) cases show unremarkable ovaries. Fallopian tube pathology included chronic salpingitis in 8 cases, hydrosalpinx in 12 cases and ectopic pregnancy in 2 cases. 69.4% of cases show unremarkable fallopian tubes (Table 3).
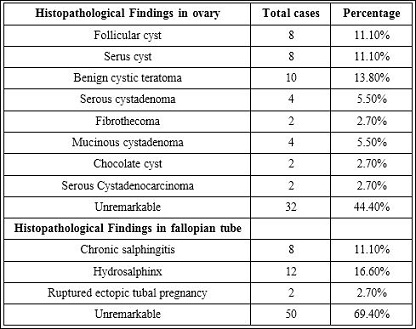
Table 3: Histopathological findings in ovaries and in fallopian tube (n=72).
Discussion
Hysterectomy is one the common surgical procedures in the peri and post menopausal women [4]. It is a successful operation in terms of symptom relief and patient satisfaction and provides definitive cure to many diseases involving uterus as well as adnexae [5]. According to the center of disease control and prevention, about five per 1000 women undergo hysterectomy annually in USA [6]. This study was conducted to analyze the patterns of lesions in hysterectomy specimens to compare findings with those of other workers. Most of the hysterectomies were performed in the age group of 40-49 years which is similar to that observed by Rather et al., [7]. It is observed that more than 90% of gynecological surgeries are performed for benign conditions with the major objective of improving the quality of life [8]. In this study 96.03% cases were benign lesion.
Hysterectomy can be performed by abdominal, vaginal or laparoscopic route. Most gynecologists around the world prefer the abdominal route [9]. The commonest surgical approach in the present study was abdominal hysterectomy. In a study by MacKanzie et al., abdominal approach was preferred in 79% cases and vaginal route in 17% cases. Similar study by Aksu et al., found 82.74% of the cases of hysterectomy done through abdominal route, which is higher than this study. The possible explanation may be due to a large number of uteroveginal prolapse cases in this present study [10,11].
The most common clinical indication in this study was menorrhagia followed by fibroid uterus. Many studies have reported menorrhagia as the most common clinical indication for hysterectomy whereas others have reported fibroid to be the commonest indication [9,12,13]. The commonest endometrial pathology observed in this study was atrophic endometrial. This is close to the observation made by Kleebkaow et al., who reported the incidence of this lesion as 3.8%. Leiomyomas of the uterus are extremely common neoplasm. The overall incidence is between 4% and 11% and occurs subserosally, intramurally, or submucosally and produce symptoms referable to their size and location [14,15]. In this study, leiomyoma was the most common pathological lesion seen in the body of the uterus of hysterectomy specimens. Similar observation was made in the studies by Abdullah [16] (34.64%). Adenomyosis is rarely diagnosed preoperatively and is still largely under diagnosed as it has no specific symptoms of its own. It is usually diagnosed after hysterectomy by histopathological examination [17]. In this study, it was the most common incidental finding on histopathological examination.
Chronic cervicitis is an extremely common condition in adult females, at least at the microscopic level. It is the commonest cervical pathology in this study, which is comparable to that reported by Talukder et al., [18]. Only four cases of malignant tumors of cervix were observed in the present study. This incidence is close to that reported by Treloar et al., [19]. Cysts of variable morphology are the most common ovarian lesions in this study. Similar results were reported in other studies [20]. Fallopian tubes are complex structures that represent more than conduits from ovary to endometrial cavity. The significance of pathologic changes in fallopian tubes is related mainly to the effect on fertility [21]. In this present study, majority of the cases revealed no pathological lesion in the fallopian tubes. The only significant lesions were chronic salpingitis, hydrosalpinx and ectopic tubal pregnancy.
Conclusion
The present study provides an insight into the histological patterns of lesions in hysterectomy specimens. A wide range of lesions was encountered on histopathological examination. Though the histopathological analysis correlates well with the clinical diagnoses, quite a few lesions are also encountered as pure incidental findings. Hence, it is mandatory that every hysterectomy specimen, even if it grossly appears to be normal, should be subjected to detailed histopathological examination to confirm various pathological lesions, better post-operative management and treatment outcome.
Competing Interests
The author declares no competing interests.
Acknowledgment
Obstetrics and Gynecology department of Jahurul Islam Medical College Hospital.
References
- Wu JM, Wechter ME, Geller EJ, Nguyen TV, Visco AG (2007) Hysterectomy rates in the United States, 2003. Obstet Gynecol 110: 1091-1095.
- Nausheen F, Iqbal J, Bhatti FA, Khan AT, Sheikh S (2004) Hysterectomy The patient’s perspective. Annals 10:339-341.
- Magon N (2012) Subtotal Hysterectomy has it come a full circle? International Journal of Clinical Cases and Investigations 4:1-4.
- Graves EJ (1992) National Center for Health Statistics: DHHS Publication (PHS) 92: 1773.
- Jaleel R, Khan A, Soomro N (2009) Clinico-Pathological study of abdominal ysterectomies. Pak J Med Sci 25: 630-634.
- Bren L (2001) Alternatives to New technologies, more options. FDA Consum 35: 23-28.
- Rather GR, Gupta Y, Bhardwaj S (2013) Patterns of Lesions in Hysterectomy Specimens: A Prospective Study. JK Science Journal of Medical Education and Research 15:63-68.
- Novak E, Berek JS (2002) Nova’’s Lippincott Williams & Wilkins, Pennsylvania, USA.
- Sobande AA, Eskandar M, Archibong EI, Damole IO (2005) Elective hysterectomy: a clinicopathological review from Abha catchment area of Saudi West Afr J Med 24: 31-35.
- MacKenzie IZ, Naish C, Rees M, Manek S (2004) 1170 consecutive hysterectomies: indications and pathology. J Br Menopause Soc 10: 108-112.
- Aksu F, Gezer A, Oral E (2004) Seventeen-year review of hysterectomy procedures in a university clinic in Istanbul (1985-2001). Arch Gynecol Obstet 270: 217-222.
- Gupta G, Kotasthane D, Kotasthane V (2009) Hysterectomy: A Clinico-Pathological Correlation Of 500 Cases. Internet J Gynaecol Obstetrics 14: 1-6.
- Shergill SK, Shergill HK, Gupta M, Kaur S (2002) Clinicopathological study of J Indian Med Assoc 100: 238-239.
- Kleebkaow P, Maneetab S, Woraluk S, Seejorn K, Thinkamrop J, et (2008) Preoperative and postoperative agreement of histopathological findings in cases of endometrial hyperplasia. Asian Pacific J Cancer Prev 9: 89-91.
- Rosai J (2011) Female reproductive systemuterus-corpus. In: Rosai and Ackerman’s Surgical Pathology. (9thedn), Elsevier, Amsterdam, Netherlands.
- Abdullah LS (2006) Hysterectomy : A Clinicopathologic Bahrain Medical Bulletin 28: 1-6.
- Shrestha A, Shrestha R, Sedhai LB, Pandit U (2012) Adenomyosis at hysterectomy: prevalence, patient characteristics, clinical profile and histopathological findings. Kathmandu Univ Med J 37:53-56.
- Talukder SI, Haque MA, Huq MH, Alam MO, Roushan A, et al. (2007) Histopathological analysis of hysterectomy Mymensingh Med J 16: 81-84.
- Treloar SA, Do KA, O’Connor VM, O’Connor DT, Yeo MA, et (1999) Predictors of hysterectomy: an Australian study. Am J Obstet Gynecol 180: 945- 954.
- Jha R, Pant AD, Jha A, Adhikari RC, Sayami G (2006) Histopathological analysis of hysterectomy specimens. JNMA J Nepal Med Assoc 45: 283-290.
- Rather GR, Gupta Y, Bardhwaj S (2013) Patterns of Lesions in Hysterectomy Specimens: A Prospective Study. JK SCIENCE 15: 63-68.
Citation: Raza AKM (2017) Histological Findings in Hysterectomy Specimens in a Tertiary Medical College Hospital in Bangladesh. J Cytol Hisitol 2: 003.
Copyright: © 2017 Raza AKM. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
