*Corresponding Author:
Andrea Pirri,
Hierarchical Medical Specialist in Sports Medicine Defense and Justice Club, Buenos Aires, Argentina
Tel: 221-4634532
E-mail: sportjavier@yahoo.com.ar
Abstract
Objectives: It is theorized that a high training/competition ratio predisposes to fewer injuries in professional footballers. This has not been studied in elite professional players.
The objective of this work was to investigate the incidence of injuries in professional players who had a frequency of one competition per week for twelve seasons. It highlights the recoverytraining cycles of five to eight days between competitions.
Method: This research is an analysis of prospectively recorded data on injuries in an Argentine professional football team, for twelve seasons.
Information on injuries was recorded daily.
Results: The evaluated team had a frequency of 3.85 competitions per month, and the ratio was 8.4 hours of training for each match hour, during the twelve years of the study. The incidence rate of injury obtained in this investigation was 4.2 per 1000 hours of training and competition.
The incidence rate of injuries in training sessions was 2.3 injuries per 1,000 hours of training. The incidence rate of injury in competition was 20.5 injuries per 1,000 hours of competition.
In 65% of all injuries players returned to competition (RTP) within seven days, with medical-kinesic treatment tailored to each athlete.
Comparison tables with European Football are presented.
Conclusions: Sports calendars with a high training/competence ratio and with a recovery/training period of 5 to 8 days between competitions, could affect a decrease in injuries that require longer RTP time and cause a relatively low incidence rate of injury in professional footballers.
Keywords
Football; Football injuries; Injury prevention; Incidence of injuries; Sports calendars
Introduction
There is a link between sports calendars and injuries. The relationship between training and competences assumes that a high training/competence ratio predisposes to fewer injuries [1]. This has not been studied in elite football players [2]. This study sought to investigate this correlation between the exposure of professional footballers to the frequency of one competition per week, with regular cycles, of 5 to 8 days, recovery-training between competitions and their incidence of injuries.
This research presents the analysis of all injuries recorded during twelve years in a Professional Football team of First, Defensa y Justicia Club, in the “Tournament National B”, of the Argentine Football Association (AFA).
Statistical analysis at the end of each season provides epidemiological data that are generally used to compare with previous seasons, with other equipment and with bibliographic data; this aims to evaluate the season and provide tools, fundamentally, of injury prevention [3-6]. UEFA (Union of European Football Associations) has expressed concern about the demands on modern footballers and the translation of these physical and mental demands into injury syndromes [2]. Theabsolute load of accumulated physical activity, in hours, which the professional footballer endures is lower among those who play a single championship and those who participate in two or more championships.
This study shows the incidence of injuries and their characteristics in a South American Professional Football team participating in a single Tournament, of 38 dates. The monthly frequency was 3.85 matches, this was low compared to other European teams that must comply with participation in two or more tournaments simultaneously, where they usually participate in 6 matches per month [7].
In elite football, some players can play up to 70 competitions per season. In the face of this frequency, players are required to play consecutive matches intermingled every 3 days and without achieving full recovery from physical performance. When the workload exceeds the athlete’s ability, it leads to excessive fatigue and an increased risk of injury [8].
This work proposes to highlight the evaluation of the organization of sports calendars and control and investigate sports seasons in professional football, for a preventive purpose.
Methods
The author of this work is a physician responsible for the professional football team, Defensa y Justicia Club base of this research. The seasons evaluated (2003 to 2012 inclusive) correspond to twelve seasons in which the team participated in the National B tournament of the Argentine Football Association (AFA). (The team also, in this period, has 7 competitions from another tournament, Copa Argentina).
The aforementioned professional was in charge of the clinical evaluation, diagnosis and treatment of the investigated equipment, a task carried out together with kinesiologists of the Club, and doctors specialized in external images.
Information about the injury was recorded, including the type, severity, site of the injury, evolution time, injury mechanism and whether it happened during a match or training.
The definition of injury was considered to be that described by J. Dvorak and A. Junge of the year 2000 of the A.J.S.M., which defines the injury as that that occurred during sports practice and that caused the athlete to absence from training/s and match/s, followed by the need for an anatomical diagnosis of damaged tissue and corresponding treatment [3-5,8,9].
In this work it was not recorded as an injury to the absence of sickness training, since, unlike other works, the non-inclusion of them could show greater specificity in relation to the epidemiology of football.
For the severity of the injury was used the concept of FIFA Medical Research Center, defined as “the length of time from when a player has incurred an injury until the day he returns for full participation in training and full availability for the competition” [3,6,10,11].
It took the recovery time of each injury until the return to football practice, the severity of the injury was determined by the number of days of absence in training [4,10]. The UEFA (Union of European Football Associations) suggests the classification: mild (1 to 3 days), less (4 to 7 days), moderate (8 to 28 days) and greater (more than 28 days) [4,11]. But for the present work was used the classification of the severity of injuries described by Dr. Vicente Paus [12] which is a modification of the classification of Dvorak and Junge, [5] based on the recovery time demanded for the return to sports activity [11,13], Grade I (mild): from 1 to 7 days; Grade II (moderate): 1 to 3.
Weeks; Grade III (severe): 3 to 8 weeks: Grade IV (severe): more than 8 weeks.
The main result of epidemiological research of sports injuries is the incidence of injuries and is usually expressed as a ratio between numerator and denominator. The numerator considers the cases (number of injuries) over a defined period of time and in the denominator the total number of athletes exposed (athletes at risk) [9]. In team sports, the incidence of injury is generally expressed in number of injuries per 1,000 hours of participation [4,8,11,14].
In many sports, exposure during competition is easy to register. However accurately recording exposure to training loads in football can be difficult [10]. This research considered, in accordance with recent studies, the incidence rate of differentiated lesions for training or matches [1,4,10,13,15].
The football teams evaluated in the twelve years were made up of an average of 28 professional players per season. The age range was 17 to 38 years, with an average age of 26 years.
All experimental procedures were designed in accordance with the Helsinki Conference for Human Research and Ethical Standards in Scientific Research in Sports and Exercise.
Results
The team evaluated had a frequency of 3.85 games per month. During the twelve years of the study, 4,710 hours of training and 715 hours of competitions were observed. The training/competition ratio was 8.4 hours of training for each match hour. This monthly and annual frequency of matches could be considered low compared to other European football teams, which participate in the local championship and in international cups.
In these 12-year follow-up years, players conducted 8317 medical consultations as part of 3364 training sessions and 461 competencies, diagnosing 797 injuries.
In these twelve seasons the standard deviation of the study was 6.31; median 68.5; the fewest injuries in a season was 53 and the highest number of injuries in a season was 73, with the range of the twelve seasons studied out of 20.
The information obtained in this research shows that the incidence rate of injury was 4.2 lesions per 1000 hours (training and competition).
The incidence rate of injuries in training sessions was 2.3 injuries per 1,000 hours of training. The incidence rate of match injuries was 20.5 injuries per 1,000 hours of competition.
The average injury absence was 21.4 hours. The injury burden was 90 days for every 1000 hours (training and competition).
The percentage of indirect contact injuries was 57.1% and by direct contact were 42.9%.
The 797 diagnosed lesions were classified according to evolution time: grade 1: 65% injuries, Grade 2 injuries: 20.82%, Grade 3 injuries: 8.53% and Grade 4 injuries: 6.02% (Graph l).
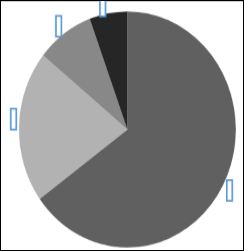
Figure 1: Return to Competition Time (RTP), (Total: 797 Injured).
65 % before 1 weeks
20.82 % between 1 and 2 weeks
8.53 % between 2 and 8 weeks
5.65% more 8 weeks
As a relevant fact, it is highlighted that in 65% of all diagnosed injuries, players returned to the competition (RTP) before seven days with medical-kinesic treatment adapted to each athlete.These include in the UEFA severity rating, to mild (1 to 3 days) and minor (4 to 7 days).
It was observed that of the 797 diagnosed lesions 355 corresponded to muscle injuries. This line found that Grade 0 muscle injury, muscle pain without DOMS anatomical injury or microscopic muscle damage [16-20]. Was the most common injury (23.84% of all injuries) and players who suffered these muscle injuries trained differently for less than a week.
Within muscle injuries, the most affected group was the posterior thigh [21] (Hamstrings) accounted for 53.46% of muscle injuries.
Data analyzed and presented in this research are compared to studies of European Football and presented in the corresponding tables 1&2.

Table 1: Incidence rate of injuries in competition and training per 1000 hours.
UEFA: “UEFA Champions League Study: A Prospective Study of Injuries in Professional Football during the 2001-2002” [16].
X: Study “Hight ratio Training/Match”.

Table 2: Player post-injury Return to Competition (RTP) before 7 days.
UEFA: UEFA Elite Club Injury Study Report 2016/17.
X: Study “Hight ratio Training / Match”.
Discussion
The objective of this research was to analyze the correlation between the exposure of professional footballers to the frequency of one competition per week, with regular periods of 5 to 8 days, of recovery-training between competition and its incidence in injuries.
In our club the epidemiology of each season, we inform it in the Medical department and in the Technical Corps. From this data we plan prevention work, which is constantly carried out. But using a stable protocol is difficult, because of the continuous change of coaches.
Data found over a twelve-season period on a professional football team could provide real data to plan sports calendars and also be able to compare with other more studied regions.
In this research the ratio was 8.4 hours of training for each hour of competition. In the UEFA 2016/17 report, the ratio was 6.3 hours of training for each hour of competition. This could mean a difference of 2.1 more hours of training per hour of championship competition developed with one date per week against championships that have periods of two dates in a week. This increased number of workouts would produce a gain from the protective effect they exert on injuries. Then, the high training/competition ratio should improve players’ fitness, protect against injuries, and generate endurance in competition [22].
In the UEFA Champions League, [15] Walden and collaborators have analyzed injury incidence levels during the tournament. The risk of competitive injury has been significantly higher in the UEFA Champions League compared to the data obtained in this study, 30.5 vs. 20.5 injuries per 1000 hours of competition, and also greater the difference from training injuries 5.8 vs 2.3 per 1000 hours of training.
In the report of the English Football Association (FA) “Injury Surveillance of the Football Association Championship 2013-2016”, the incidence of competition and training injuries were also higher than data found in this study, 23.8 vs 20.5 injuries per 1000 hours of competitions and also higher the incidence of training injuries 4 vs 2.3 injuries per 1000 hours of training.
This study found, in relation to the severity of injuries, a high proportion, 65%, of injuries with player returns to competition (RTP) before 7 days. This proportion was above what was reported in other European Football studies [1,3,5,15,21,23,24] In the UEFA Elite Club Injury Study Report 2016/17 the RTP before 7 days was 27.1%. While in the 16-year analysis of the UEFA Elite Club Injury Study, rtp before 7 days was 42% [24].
Therefore we can express that in this study most absences from injuries were attributed to diagnoses of minor injuries. The combination of the frequency and severity of the injury, i.e. the burden of injury burden, is probably a clinically considered tool to describe the impact of injuries on professional football teams [25]. In this study the injury load was 90 days per 1000 hours (training and competition). In the 11-year-old Studio of Hagglund and Ekstrand of the UEFA Champions League, the injury burden was higher than this study, 130 days /1000 hours [26].
It was also observed that the incidence rate of injury (4.2 per 1000 hours) was low compared to other European Football studies [1,4,15,27].
These observed data would relate to the fact that the twelve years of the study coincided with regular seasons of 38 official matches, with recovery-training periods of 5 to 8 days between competencies, with two annual competition cycles, two preparatory periods and two transition periods; unlike most European football that cover an average of 60 matches with a period of competition, a preparatory period and a transition period.
This study would show that the regularity of official parties with a recovery period of 5 to 8 days between matches and an adequate training-competence ratio could affect a lower proportion of injuries requiring longer recovery time, and a relatively low incidence rate of injury [15,25].
The application of protocols for the prevention of injuries in high performance is considered to be fundamental [3,5,10,28] and this work could show that within these protocols a ratio of 8.4 training/ competence could be a preventive factor of injury in professional football. It would be desirable in future research to find the right amount of skills and trainings in relation to the annual schedule.
The data in this research provide useful information to proactively work on the development and planning of sports calendars in relation to injury prevention.
References
- Bengtsson H, Ekstrand J, Hägglund M (2013) Muscle injury rates in professional football increase with fixture congestion: An 11-year follow-up of the UEFA Champions League injury study. Br J Sports Med 47: 743-
- Ekstrand J, Waldén M, Hägglund M (2004) A congested football calendar and the wellbeing of players: Correlation between match exposure of European footballers before the World Cup 2002 and their injuries and performances during that World Br J Sports Med 38: 493-497.
- Fuller CW, Ekstrand J, Junge A, Andersen TE, Bahr R, et (2006) Consensus statement on injury definitions and data collection procedures in studies of football (soccer) injuries. Br J Sports Med 40: 193-201.
- Belloch LL, Figueres LL, Soriano P (2010) The epidemiology of football: A systematic review. Int J Spo-Rel Med Sci 10: 22-40.
- Dvorak J, Junge A, Grimm K, Kirkendall D (2007) Medical report from the 2006 FIFA World Cup Germany. Br J Sports Med 41: 578-581.
- Drawer S, Fuller CW (2002) Assessing the level of injuries in English professional football through a risk-based assessment process. Br J Sports 36: 446-451.
- Ekstrand J, Hägglund M, Waldén M (2011) Injury incidence and injury patterns in professional football: The UEFA injury Br J Sports Med 45: 553-558.
- Gabbett TJ (2016) The training-injury prevention paradox: Should athletes be training smarter and harder? Br J Sports Med 50: 273-280.
- Hagglund M, Walden M, Bahr R, Ekstrand J (2005) Methods for epidemiological study of injuries to professional football players: Developing the UEFA model. Br J Sports Med 39: 340-346.
- Cosa F, Cosb MA, Buenaventurac L, Prunad R, Ekstrand J (2010) Analysis models for the prevention of sports injuries. Epidemiological study of injuries: The UEFA model in Apunts Sports Mesicine 45: 95102.
- Fuller CW, Junge A, Dvorak J A six year prospective study of the incidence and causes of head and neck injuries in international Br J Sports Med 39: 3-9.
- Pas V, Torrengo F (2006) Incidence of Injuries in Professional Football Players. Argentine Sports Traumatology Association Magazine 10: 10-17.
- Dvorak J, Junge A, Chomiak J, Graf-Baunmann T, Peterson, L, et al. (2000) Risk Factor Anallysis for Injuries in Football Player. AJSM 28: 40-46.
- Hägglund M, Waldén M, Ekstrand J (2006) Previous injury as a risk factor for injury in elite football: A prospective study over two consecutive Br J Sports Med 40: 767-772.
- Waldén M, Hägglund M, Ekstrand J (2005) UEFA Champions League study: A prospective study of injuries in professional football during the 2001-2002 season. Br J Sports Med 39: 542-546.
- Ekstrand J, Healy JC, Waldén M, Lee JC, English B, et (2012) Hamstring muscle injuries in professional football: the correlation of MRI findings with return to play. Br J Sports Med 46: 112-117.
- Valle X, Alentorn-Geli E, Tol JL, Hamilton B, Garrett Jr WE, et al. (2017) Muscle Injuries in Sports: A New Evidence-Informed and Expert Consensus-Based Classification with Clinical Application. Sports Med 47: 1241-1253.
- Evans GF, Haller RG, Wyrick PS, Parkey RW, Fleckenstein JL (1998) Submaximal delayed-onset muscle soreness: Correlations between MR imaging findings and clinical measures. Radiology 208: 815-820.
- Pollock N, James SL, Lee JC, Chakraverty R (2014) Br J British Classification of Athletic Muscle Injuries: A New Classification Sports Med 48: 1347-1351.
- Verrall GM, Slavotinek JP, Barnes PG, Fon GT (2003) Diagnostic and prognostic value of clinical findings in 83 athletes with posterior thigh injury: Comparison of clinical findings with magnetic resonance imaging documentation of hamstring muscle strain. Am J Sports Med 31: 969-973.
- Krutsch W, Eder K, Krutsch V, Meyer T, et “Stay and play” in football: Art of keeping players fit to play. Unfallchirurg 121: 433-440.
- Stevens TGA, de Ruiter CJ, Twisk JWR, Savelsbergh GJP, Beek PJ (2017) Quantification of in-season training load relative to match load in professional Dutch Eredivisie football players. Sci Med Footb 2: 117-125.
- Hägglund M, Waldén M, Ekstrand J (2013) Risk factors for lower extremity muscle injury in professional soccer: The UEFA Injury Am J Sports Med 41: 327-335.
- Ekstrand J, Krutsch W, Spreco A, van Zoest W, Roberts C, et al (2020) Time before return to play for the most common injuries in professional football: A 16-year follow-up of the UEFA Elite Club Injury Study. Br J Sports Med 54: 421-426.
- Bahr R, Clarsen B, Ekstrand J (2018) Why we should focus on the burden of injuries and illnesses, not just their incidence? Br J Sports Med 52: 1018-1021.
- Hägglund M, Waldén M, Magnusson H, Kristenson K, Bengtsson H, et al. (2013 Injuries affect team performance negatively in professional football: An 11-year follow-up of the UEFA Champions League injury Br J Sports Med 47: 807-808.
- Junge A, Chomiak J, Dvorak J (2000) Incidence of football injuries in youth Comparison of players from two European regions. Am J Sports Med 28: 47-50.
- McCall A, Dupont G, Ekstrand J (2016) Injury prevention strategies, coach compliance and player adherence of 33 of the UEFA Elite Club Injury Study teams: A survey of teams’ head medical Br J Sports Med 50: 725-730.
Citation: Lacki JF (2021) High Training/Competition Ratio, Less Incidence of Injury? Professional Football Epidemiological Exploration. J Emerg Med Trauma Surg Care 3: 011
Copyright: © 2021 Lacki JF. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and re- production in any medium, provided the original author and source are credited.