*Corresponding Author:
Stefano Sechi,
“ParideStefanini” Department Policlinico “Um- berto I”, “Sapienza” Università di Roma, 00185 Rome, Italy
Tel: +39 0633775593
Fax: +39 0633776317
Email: s.sechi@uniroma1.it
Abstract
Here we present you a Type II of Crawford classification aortic aneurysm. Our patient 89-year-old woman with history of hypertension, diabetes mellitus, smoking habits and polyposis of descending/sigmoid colon came to our attention for rectorrhagia, asthenia, dyspnoea and dizziness.
A computer tomography exam revealed an aortic arch aneurysm, aortic ectasia at a level of aortic hiatus and infra-renal aortic aneurysmal dilation.
In accord to aortic team meeting and patient decision, to refer this lady to medical therapy instead to surgery/hybrid treatment for age patient, comorbidities and high mortality relates to intervention. Aortic arch pathologies are unusual and their treatment is challenging.
The aetiology of aortic arch diseases is congenital, chronic, post traumatic, inflammatory, infectious, mechanical and anastomotic, but most frequently is degenerative. Furthermore, the improvement in diagnostic imaging and the aging populations, aortic arch aneurysms have increasingly diagnosed.
The incidence of aortic arch diseases is 10-11% and many patients were asymptomatic. Otherwise, many patients came to hospital with catastrophic, life-threatening events and urgent treatment is required.
Despite the progress and new technologies have produced new therapeutic options for both cardiac and vascular surgeons is important to highlight the primary role of the aortic team, an interdisciplinary assessment, to find the best tailored treatment, both in acute and chronic setting, for the interest of each patient.
Keywords
Aorta; Aortic; Arch aneurysm
Case Presentation
We report a case of an 89-year-old woman with a past medical his- tory of hypertension, diabetes mellitus, smoking habits, and polyposis of descending and sigmoid colon. She came to our attention for rec- torrhagia, asthenia, dyspnea and dizziness within the last 4 days.
A total body Computer Tomography (CT) was made at the admis- sion. The exam revealed giant distal aortic arch aneurysm (12 cm), aortic aneurysm at level of aortic hiatus and infra-renal aortic aneu- rysm (Figure 1) (Type II of Crawford classification) with no signs of rupture or dissection nor evidence of bleeding. There are compression phenomena of the esophagus, trachea, left pulmonary artery and low- er lobe of the left lung (Figure 2). The aetiology of this specific case is very likely atherosclerotic.
In accord to aortic team meeting and patient decision, we refer this lady to medical therapy instead surgery/hybrid treatment for age patient, comorbidities and high mortality relates to intervention and led a follow-up with CT scan exam every twelve months.
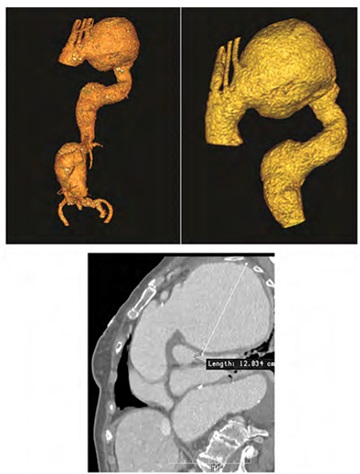
Figure 1: Computer tomography 3D reconstruction of Crawford Type II aortic aneurysm. Maximum diameter was 12 cm at level of aortic arch.
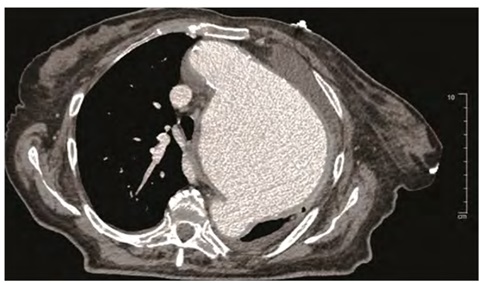
Figure 2: Computer tomography image showed compression phenomena of the left thoracic structures.
Discussion
Aortic aneurysm is defined as a permanent focal or extensive dilatation of the aorta that involves all layers of the aortic wall with a diameter of the vessel is at least 50% greater than the normal size. The aetiology of the aortic arch aneurysm is varied. The main causes are congenital, post traumatic, inflammatory, infectious, mechanical and anastomotic, but most frequently is degenerative [1].
The aortic arch aneurysms have been increasingly diagnosed for the incremental usage of diagnostic imaging and the increase aging populations, but there is no controlled trial either prior study that spe- cifically looked at the natural history and the expansion rate of aortic arch disease [2].
Risk factors for growing aortic diameter include age, female gen- der, chronic obstructive airway disease, hypertension, aortic diameter and a family history of aneurysms. The progressive increment of aor- tic arch size is often asymptomatic process and may lead to various scenarios. The worst complications represent the rupture and dissec- tion. Davies and co workers reported an aorticexpansion rate of 1 mm per year and a yearlyrupturerisk of 6.9% in aneurysms with more than 6 cm of diameter [3].
Yiu, et al. in their study showed, in a cohort of 45 patients, an aneu- rismal growth rate about 2.5 mm per years with 22% of aneurysm rup- ture in relationship with maximum diameter of 6.5 cm and also with hyperlipidemia [4].
It is important to underline that growth rates vary according to the underlying disease and the absolute size of the aneurysm and risk of aneurysm rupture increases generally with aneurysmsize. The prevalence of aortic aneurysms in the general population is difficult to determine because of under estimated of these aneurysms in mortality statistics. In 2002, the prevalence was 16.3 per 100,000 per year for men and 9.1 per 100,000 per year for women [1,5].
The most common anatomical location of thoracic aortic aneury- sms is the ascending aorta and/or aortic root in 51% of cases, while the descending aorta is affected in approximately 38%. Specifically the incidence of aortic arch diseases is 11% and many patients were as- ymptomatic [6,7].
Otherwise, many patients came to hospital with catastrophic, life-threatening events and urgent treatment is required [1]. Prog- ress and new technologies have produced new therapeutic options for both cardiac and vascular surgeons. The treatment of aortic arch disease may be surgical, hybrid repair or endovascular repair but it remains challenging [8,9].
Preoperative management of aortic arch pathology and risk strati- fication for each patient allow to take the best treatment choice.
In the literature some case reports showed an aortic arch aneurysm that was treated by surgical or hybrid/interventional fashion. Hela, et al. reported a case of 77-years old woman affected by ascending aorta and aortic arch aneurysm with a maximum diameter of 13.97 cm at- level of ascending aorta without history of hypertension and cardiac symptoms or family history. This patient was treated by open surgery. Their patient died 4 days after surgery by multi-organ failure [7].
Desai, et al. in their work showed a 54-year-old man with 12 cm fusiform aneurysm of the distal aortic arch. Open surgery was made and the patient was discharged on the 10th post operative day without complications [10].
Saito and coworkers reported a 86-year-old woman referred for aortic arch aneurysm with a maximum diameter of 11 cm. For pa- tientage, they decided to treat this patient by endovascular repair.
The patient required prolonged hospitalization becouse of musco- lar atrophy by age and disuse [11]. Zhou, et al. reported a combined approach of open surgical debranching followed by antegrade stent grafting to treatthe rest of aortic disease [12].
In our report the patient decided to not undergo anysurgical or interventional treatment. In addition comorbities and clinical pre- sentation made a very high operative risk of mortality and morbidity. Moreover, our case showed one of the biggest distal aortic arch aneu- rysm in literature.
The improvement of surgical techniques had made open surgery more safely and decreased the perioperative morbidity and mortality rate, but new endovascular solutions in the treatment of aortic pathol- ogies continue to improve the applicability of these techniques to each specific patient anatomies. In conclusion, is important to highlight the primary role of the aortic team, an inter disciplinary assessment, to find the best tailored treatment, both in acute and chronicsetting, for the interest of each patient.
References
- 1. Kouchoukos NT, Kirklin JW (2013) Kirklin/Barratt-Boyes cardiac surgery: Morphology, diagnostic criteria, natural history, techniques, results, and indica- Elsevier/Saunders, Pennsylvania, USA.
- 2. Czerny M, Schmidli J, Adler S, van den Berg JC, Bertoglio L, et al. (2019) Current options and recommendations for the treatment of thoracicaortic pa- thologies involving the aortic arch: An expert consensus document of the Eu- ropean Association for Cardio-Thoracic Surgery (EACTS) and the European Society for Vascular Surgery (ESVS). Eur J Cardiothorac Surg 55: 133-162.
- 3. Davies RR, Goldstein LJ, Coady MA, Tittle SL, Rizzo JA, et (2002) Yearly rupture or dissection rates for thoracic aortic aneurysms: Simple prediction based on size. Ann Thorac Surg 73: 17-27.
- 4. Yiu RS, Cheng SW (2016) Natural history and risk factors for rupture of tho- racic aortic arch aneurysms. J Vasc Surg 63: 1189-1194.
- 5. Cheng SWK (2016) Aortic arch pathologies-incidence and natural Gefasschirurgie 21: 212-216.
- 6. Isselbacher EM (2005) Thoracic and abdominal aortic Circulation 111: 816-828.
- 7. Hela BJ, Nesrine G, Taieb C, Abdessalem H, Aiman D, et al. (2016) Giant ascending aortic aneurysm complicated by a tracheal compression: A case report and review of the literature . J Clin Exp Cardiolog 7.
- 8. Rommens KL, Estrera AL (2019) Contemporary management of aortic arch Semin Thorac Cardiovasc Surg 31: 697-702.
- 9. Cazavet A, Alacoque X, Marcheix B, Chaufour X, Rousseau H, et al. (2016) Aortic arch aneurysm: Short- and mid-term results comparing open arch surgery and the hybrid procedure†. Eur J Cardiothorac Surg 49: 134-140.
- 10. Desai D, Kothari J, Brahmbhatt B (2019) Management of intact giant fusiform aneurysm of distal aortic arch with impeding risk of rupture using midline ster Indian Journal of Vascular and Endovascular Surgery 6: 320-323.
- 11. Saito N, Kimura T, Toma M, Kita T, Inoko M, et (2005) Images in cardiovascular medicine. Endovascular treatment of a giant aortic arch aneurysm with a triple-branched stent graft. Circulation 112: 151-152.
- 12. Zhou W, Reardon ME, Peden EK, Lin PH, Bush RL, et al. (2006) Endovascular repair of a proximal aortic arch aneurysm: a novel approach of supra-aortic debranching with antegrade endograft deployment via an anterior thoracoto my approach. J Vasc Surg 43: 1045-1048.
Citation:Sechi S, De Luca A, Dezi T, Taurino M, Sinatra R (2020) Giant Aortic Arch Aneurysm in Elderly Patient. J Case Repo Imag 4: 028.
Copyright: © 2020 Sechi S, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
