*Corresponding Author:
Laachoubi Mohamed,
Department of Otorhinolaryngology, Head and Neck Surgery, King Université Hassan II, Casablanca, Morocco
Tel: +212 621376953
Email: med.laachoubi@gmail.com
Abstract
Meningiomas are benign tumors originating from the arachnoid villi of the meninges. Meningiomas extending to the internal auditory canal are very rare and can imitate serous otitis media with a highrisk of misdiagnosis. The diagnosisis based on an evaluation of imaging with computed tomography and magnetic resonance imaging. This short report aims to warn the otolaryngologist of this rare situation to preventany delay to find out the correct diagnosis of intracranial meningioma. we report a case of unilateral chronic serous otitis revealing underlying meningioma in a 43 year old women patient.
Keywords
Internalauditory canal; Meningiom; Serousotitis media; Skull base
Introduction
Meningiomais the second most common tumor from the cerebellopontine angle, after the vestibular schwannoma, representing less than 5% of tumors in this region [1]. Most posterior cerebral fossa meningiomas arise at the posterior face of the petrous bone and some may extend into the internal auditory canal [2]. The clinical symptoms are similar to those of vestibular schwannomas and manifest as hearing loss, tinnitus, vertigo or facial nerve weakness. Serous otitis media secondary to eustachian tube obstruction has also been reported [3-4].
Case Report
A 43 year old women was presented to our ENT department with hearing loss and tinnitus in her left ear which had begun 8 months earlier. She had no facial paresis.
Otoscopy revealed fluid behind an intact left tympanic membrane suggesting serous otitis media (Figure 1).

Figure 1: Serous otitis media of the left ear.
There were no neurological symptoms or deficits and endoscopy showed a normal nasopharynx. Audiometry showed mixed conductive and sensorineural hearing loss (Figure 2).
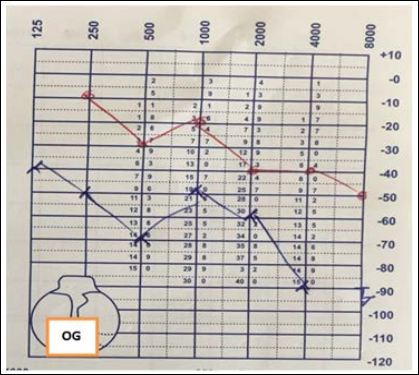
Figure 2: Mixed left hearing loss.
The MRI with gadolinium revealed the presence of a large multilobed lesion of the base of the skull in iso signal T1 and hypersignal T2, intensely enhauced, measuring 51*50*44 mm. This lesion includes the posterior part of the sphenoid sinuses and the internal carotid arteries. It also extended to the left internal auditory canal. These imaging findings were consistent with the diagnosis of meningioma (Figure 3).
The patient was referred to the neurosurgery department for management.
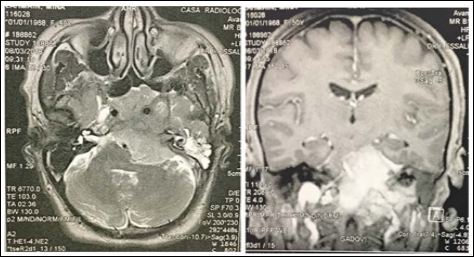
Figure 3: Coronal and axial T1-weighted magnetic resonance showing homogeneous gadolinium enhancement of an extensive meningioma.
Meningiomas are benign tumors arise from the dural coverings of the brain. They are slowly growing benign tumors which account for 20% of intracranial tumors [5].
According to WHO 2016, meningiomas are classified into 3 grades: 81.1% are grade I (typical), 16.9% are grade II (atypical) and1.7% are grade III (anaplastic) [6].
The peak of occurrence is around the fifth decade but the diagnosisis made the most often between the ages of 20 and 60.
Meningiomas extending into the mastoid or middle ear has been described and can imitate serous otitis media with a highrisk of misdiagnosis. Ayache et al. described a series of patients with temporal meningioma whose main symptoms suggested serous otitis media [7].
In the literature three main access routes to the temporal bone. Intracranial meningiomas most often spread in the internal auditory canal, often invading the innerear, the second routeisa direct transosseous spread through the mastoidor the middle earcavity of an intraosseous meningioma. The last routeis the result of an obstruction of the eustachian tube due to the extension of the tumor in the cavity of the middle ear [8].
In some cases, a secretory-type meningioma or a cerebrospinal fluid leak in the tympanic space is found to be responsible for serousotitis [9].
The clinical symptoms of intracanalicular meningiomas are very similar to those of vestibular schwannomas causing sensorineural deafness, tinnitus, dizziness or facial palsy.
MRI scans contrast enhancement and Computed tomography scans in the internal auditory canal determine the diagnosis and extent of meningioma. On T1-weighted images meningioma are mostly isointenseor slightly hypointense to the white matter. And hypointense or isointense on T2-weighted images. Whereas meningiomas tend to be hyperintense. An intense enhancement is observed after gadolinium injection [8].
The classic approach is complete surgical excision as this offers the highest chance of survival. Total resection would result in overall fiveyear survival a rate of around 85%. The prognosisis generally good, but remains marked by a highrisk of recurrence requiring regular surveillance [10].
Conclusion
Any unilateral hearing failing, isolated tinnitus, hearing loss, progressive or sudden installation, recent or old, justifies an investigation, looking for an expansive process of the posterior cerebral fossa, particularly of the internal auditory canal or cerebellopontine angle.
Computed tomography in conjunction with MRI establises the diagnosis. This short report aims to warn the otolaryngologist of this rare situation to preventany delay to find out the correct diagnosis of meningioma.
References
- 1.Brackmann DE, Bartels LJ (1980) Rare tumors of the cerebelloton- pine angle. Otolaryngol Head Neck Surg 88: 555-559.
- 2.Atlas MD, Fagan PA, Turner J (1992) Calcification of internalaudito- ry canal tumors. Ann Otol Rhinol Laryngol 101: 620-622.
- 3.Chang CY, Cheung SW, Jackler RK (1998) Meningiomas present- ing in the temporal bone: The pathways of spreadfrom anintracrani- al site of origin. Otolaryngol Head Neck Surg 119: 658-664.
- 4.Civantos F, Ferguson LR, Hemmati M, Gruber B (1993) Temporal meningiomas presenting as chronicotitis Am J Otol 14: 403- 406.
- 5.Whittle IR, Smith C, Navoo P, Collie D (2004) Meningiomas. The Lancet 363: 1535-1543.
- 6.Ostrom QT, Gittleman H, Xu J, Kromer C, Wolinsky Y, et (2016) CBTRUS statistical report: Primary brain and other central nervous system tumors diagnosed in the United States in 2009-2013. Neuro Oncol 18: 1-75.
- 7.Ayache D, Trabalzini F, Bordure P, Gratacap B, Darrouzet V, et al. (2006) Serousotitis media revealing temporal en plaque meningio- Otol Neurotol 27: 992-998.
- 8.Hamilton BE, Salzman KL, Patel N, Wiggins RH, Macdonald AJ, et (2006) Imaging and clinical characteristics of temporal boneme- ningioma. AJNR Am J Neuroradiol 27: 2204-2209.
- 9.Keereweer S, Metselaar RM, Dammers R, Hardillo JAU (2011) Chronic serous otitis media as a manifestation of temporal meningi- ORL J Otorhinolaryngol Relat Spec 73: 287-290.
- 10.Marosi C, Hassler M, Roessler K, Reni M, Sant M, et al. (2008) Meningioma. Crit Rev Oncol Hematol 67: 153-171.
Citation:Laachoubi M, Beghdad M, Mallouk S, Oukessou Y, Rouadi S, et al. (2020) Extensive Meningioma of the Posterior Cerebral Fossa Presenting as a Serous Otitis Media. J Case Repo Imag 4: 021.
Copyright: © 2021 Laachoubi M, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
