*Corresponding Author:
Silvério-Lopes S,
IBRATE Technology College Brazil
Email: san.silverio@yahoo.com.br
Abstract
Background: Spiral Cord Injury (SCI) is a great concern and challenge for the professional’s involved, patient, family and for the State. As much as modern science has evolved in recent years, the spinal cord injured patient still suffers from the limitations imposed by the losses, some of them irreparable. Acupuncture has been discreetly occupying space in the neurological area; I still have a great need for research and understanding.
Aim: Draw the energy profile of the meridians of SCI patients.
Methodology: 30 individuals with paraplegia aged 18 to 72 years (mean ± 41.83 years); 57% men and 43% women, recruited from patients at the Hospital of the State University of Londrina (Brazil). They were evaluated by the Ryodoraku technique, with electrodiagnostic equipment of the brand NKL; model OMNIPAX before the usual physiotherapy sessions. Demographic, historical and ASIA Impairment Scale (AIS) data from each patient’s records were used directly from the clinic’s database. Research Ethics Committee No.1556794.
Results: AIS-A (53%), AIS-B (19%), AIS C (28%) profile. Sample’s bioimpedance mean was 26 µA. 86% of the population had an energy imbalance, with an average of 74% of these being characteristic of a deficiency pattern. There were also changes in the Ryodoraku cartography traces, typical “high-low” imbalances in 67% of the sample.
Conclusion: Energy imbalance due to deficiency, preferably reaching the Bladder (BL), Gallbladder (GB), Kidney (KI), Spleen (SP) meridians.
Keywords
Acupuncture; Ryodoraku electrodiagnosis; Spinal cord injured
Introduction
Spinal Cord Injury (SCI) is a neurological syndrome characterized by an injury to the spinal cord that causes its partial or total interruption, which can cause neurological damage and neurovegetative disorders below the level of the injury with changes in motor, sensory and autonomic functions, as well as consequences in other systems [1].
In a study with more than 100 articles evaluated, it was concluded that the global incidence of spinal cord injuries was 10.5 cases per 100,000 people, resulting in an estimated number of 768,473 new cases annually worldwide [2].
After a SCI, a situation of disability determines a variety of changes both in the life of the person affected and that of his family members [3]. Aspects with the highest impact in the quality of life of patients with spinal cord injury are those considered negative changes in the domains: physical, psychological, social, including, sexual activity and pain [4].
The individual with SCI may have paraplegia, which is when he presents only lower limb movements, or a quadriplegia where there is no movement of the upper limbs or lower limbs. To express the degree of neurological impairment of the individual with SCI, the American Spinal Injury Association standardized the ASIA Impairment Scale (AIS) based on the assessment of the preservation or not of aspects of motor and sensitivity [5].
The patient with SCI has neurophysiological changes that result from the total and/or partial interruption of nerve conduction. The speed of nerve conduction is decreased or absent in these patients. However, modern studies demonstrate levels of somatosensory preservation even in injuries considered before, as complete [6]. These findings open up promising paths to future possibilities in the neurological field.
The SCI patient is traditionally treated with physiotherapy, and is rarely seen by Complementary Alternative Medicine (CAM). It is also unusual for it to be the focus of scientific research in the naturist area. Acupuncture structured its therapeutic bases in a period of history in which current neuro-physiological knowledge was not available, where energy meridians were described as “channels where vital energy circulates” called Qi.
There have been great advances in the establishment of acupuncture as a therapeutic resource, especially for analgesia [7] anxiety disorders [8] comorbidities such as obesity [9] chemical dependency [10], among others. Advances also in scientific proof of the mechanisms of action of acupuncture [11,12].
On the neurological field, acupuncture has shown effectiveness in treating some types of sequelae, such as Parkinson’s [13], Facial Paralysis [14]. Classical Chinese acupuncture has as its basic theories the study of energy meridians. However, it is not yet conclusive how this vital energy conduction system presents itself to the SCI patient.
In view of this concern, the present study aim was to trace the energy profile of the meridians of SCI patients using a technological resource of the Ryodoraku electrodiagnosis.
Ryodoraku electrodiagnosis from the point of view of physics indirectly assesses the electrical resistance of the skin in certain acupoints, by measuring the circulating electrical current.
Methodology
Recruitment and selection of participants
Participants were recruited from patients who attended the neurological physiotherapy service at Hospital from Londrina State University (Brazil). Inclusion criterion was to present spinal cord injury of the spastic or flaccid paraplegia type, older than 18 years of age, not to have lesions or dermatological changes in the wrist and ankle regions (places of inspection of the technique), not to have a pacemaker. Sexes, races, religion and color were included. Individuals with quadriplegia and paraparesis were excluded.
Sample
The study included initially 34 individuals who had SCI. Of those, 2 were excluded by technical criteria and 2 by withdrawal. Sample consisted in 30 volunteers, the sample was characterized by individuals of both sexes, being 57% men and 43% women with ages between 18 and 72 (mean±41, 83 age), with spastic or flabby paraplegia. The sample size was intentional, not probabilistic.
Materials and Methods
Digital Ryodoraku electrodiagnostic equipment branded NKL, model OMNIPAX, registration with the National Health Surveillance Agency (ANVISA) n° 80191680005. Saline with 0.9% NaCl, hydrophilic cotton, anatomical forceps, software for drawing up the Ryodoraku graph, brand Kimeter version 2.1. Demographic, historical and ASIA Impairment Scale (AIS) data from the records of each patient were used directly from the database of the Hospital from the Londrina State of University (UHLSU).
Procedures
Records of patients undergoing treatment were separated in the clinic’s database to previously select the sample according to the inclusion and exclusion criteria. Then, a verbal invitation was made to the patient by one of the researchers, where the objectives of the study and procedures were explained. With agreement and interest, patient signed a Free and Informed Consent Form (FICF) and Ryodoraku technique data collection was scheduled for the following day, before their physiotherapy consultation.
Data collection followed Nakatami’s original Ryodoraku electrodiagnostic technique [15], where socks, shoes, watches, bracelets; rings were removed initially, because they could tighten the wrist and ankles. The patient was at rest for 10 minutes sitting in his wheelchair.
The reading started with the points recommended by the technique on the upper limb (right and left wrists), and then on the lower limbs (ankles/right and left feet) as shown in Figure 1.

Figure 1: Reading the Ryodoraku electrodiagnosis in acupuncture.
Ethical aspects
The study followed the ethical standards of the Declaration of Helsinki, having been approved by a Research Ethics Committee under the protocol n° 1.556.794, and , and registered in the Brazilian Registry of Clinical Trials RBR-7 on march 9, 2020. http://www. ensaiosclinicos.gov.br/rg/RBR-7jwxqd/
Statistical treatment
The data presented in the results were based on individual collections. There was no exclusion of samples. Calculations were by simple arithmetic average and percentage calculations.
Results
As for the severity profile of the sample’s neurological injury, according to the ASIA Impairment Scale (AIS), the predominance of patients classified as AIS A was found. Based on the fact that the sample was intentional and non-exclusive, it is deduced that the majority of patient’s attending the physiotherapy service had a complete motor and sensory injury. Table 1 summarizes the results for the sample profile.
The sample was characterized by individuals of both sexes, being 57% men and 43% women with ages between 18 and 72 (mean±41, 83 age), with spastic or flabby paraplegia.
Group’s mean for injury time was 14 years and 2 months. As for the profile of the neurological injury according to the ASIA Impairment Scale (AIS), they were classified as AIS-A (63.3%), AIS-B (16.7%), AIS-C (20%).
Average circulating current of the sample was 26 µA. The percentage of the group that presented energy imbalance according to the Ryodoraku electrodiagnostic assessment was 86%. The vast majority of imbalances were of the energy deficiency type (74% of the imbalances).
Energy meridians that most appeared in imbalance were Bladder (BL), Gallbladler (GB), Spleen (SP) and Kidney (KI), whose sum makes up 50% of all imbalances.
There were also important changes in the Ryodoraku mapping, typical “high-low” imbalances in 67% of individuals.
For the sake of illustration, in Figure 2 is shown a graph of the Ryodoraku electrodiagnosis of one of the patients in the sample, with an energy deficiency pattern.
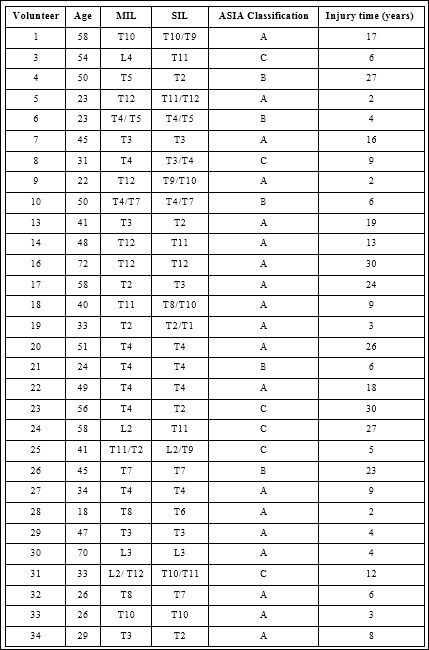
Table 1: Data from volunteers in age, Motor Injury Level (MIL), Sensitive Injury Level (SIL), ASIA Impairment Scale (AIS) classification, and injury times.
L= Lumbar vertebra; T= Thoracic vertebra
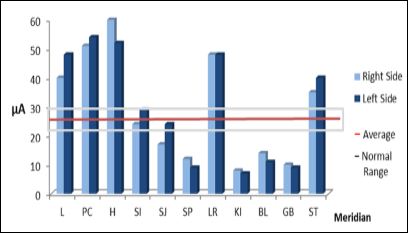
Figure 2: Illustration of Ryodoraku chart in columns by one of the volunteers.
There was no relationship between the ASIA Impairment Scale and energy changes
Discussion
In this study, the sample had a slight predominance of men, in which 57% of men and 43% of women were evaluated. The epidemiological survey carried out in Ireland by Smith et al., [16] indicates a prevalence of men with SCI in that population in the order of 75.4%.
A study developed in Czech Republic [17] highlights similarly a majority of men with this type of lesion. Predominance is probably justified due to the fact that falls from a great height, firearms and automobile accidents are among the etiological factors of SCI, which men are exposed to proportionally more than women.
Group’s mean for injury time was 14 years and 2 months. The shortest injury time was two years, found in 3 volunteers. However, there were no correlations between the time the injury was present and the energy imbalances assessed by the Ryodoraku electrodiagnosis.
In this study, the average electrical current of the group, measured by the ohmmeter in the acupoints of the Ryodoraku technique, was 26 µA, suggesting it to be low. This result is consistent with another study that showed a gradual decrease in the circulating electrical current measured by the Ryodoraku technique in patients with Parkinson’s with increasing levels of severity [18].
Circulating energy in the human body depends on several factors, being considered a cellular phenomenon. At the end of the last century, physics and biology came together in an attempt to understand the phenomena that permeate the human body. New terminologies have emerged, including bioenergetics that designates the study of forms of energy and their interconversions in the context relevant to biological systems, living organisms [19].
A study by Jingjing Y et al., [20] cites that there are research from several fields (biochemistry, electromagnetic, biophysics) showing evidences that support the existence of acupuncture channels and points. Studying the nature of acupuncture meridians, Ahn et al.,[21] describes and associates them to collagen bands, representing high echogenicity at ultrasound that seem to be associated with high impedance.
If you assume that the ohmmeter has a constant voltage, when the electrode takes the electrical stimulus, what is measured is the circulating current that runs through the body. Impedance (Z), in turn, will be due to all the morphological components of the body through which the electric current passes. In the case of a low electric current output measured by the Ryodoraku technique in this study it means that it found a higher impedance, which in the case of biological systems includes Resistance (R) and Capacitive Reactance (Xc) [22]. As for the characteristics of the energy profile within the understanding of acupuncture, 86% of the sample presented imbalances. This means that at least one of the energy meridians was altered. The vast majority of energy imbalances (74%) were energy deficiency.
This result is relevant, since the lack of vital energy, resulting from the injury, especially in the lower limbs, will be reduced by the lower blood supply, infiltration of muscle fat, deficit in muscle strength, contractures, hypotonia and lymphatic compromises among others [23].
Energy deficiencies, characteristics of SCI, found in this study by the Ryodoraku electrodiagnosis may reflect a high resistance to the passage of electric current. It is suggested that it may be due to the absence of nerve stimulation in the lower limbs, less water in the tissues, poor depolarization at the level of the cell membrane, and the collagen bands of the meridians, functioning as a bad conductor.
Twelve main meridians are symmetrical, with six running through the upper limbs and another six running through the lower limbs. In the present study it was observed that the most compromised meridians Bladder (BL), Gallbladder (GB), Kidney (LI) and Spleen (SP), have their path in the lower limbs that, in the case of the studied patients, do not move due to SCI. Two of these meridians are descendants and two are ascendants. However, Stomach (ST) and Liver (LV) that also travel through the lower limbs have not changed.
Correlations that can be made with these results are still poor, such as associating the deficiencies of the GB and SP meridians because they are in the acupuncture theories responsible for the tendons and muscles respectively. Since there is a lack of movement in the lower limbs in the SCI, this energetic function would be compromised.
There is no way to list the compromised meridian as the source of the pathology, or energy syndrome since it is of traumatic origin. However, knowing which of these meridians have been impaired can lead to an understanding of the energy compromises arising from disruptions and biomechanical immobility present in SCI.
As a limitation of the present study, it was found that there were many variables that would need to be better grouped, such as injury time, classification by the ASIA Impairment Scale, the type of sequel as well as the comorbidities associated with the patient with SCI.
Conclusion
In this study, average circulating electrical current of the group, measured by the ohmmeter in the acupoints of the Ryodoraku technique, was 26 µA, demonstrating that even with the interruption of nerve conduction in SCI, other biological structures still exist which offer a means of conducting residual current (low).
The present study also concluded that the profile of the population of SCI patients was characterized by an imbalance of the energy deficiency type, reaching primarily the Bladder (BL), Gallbladder (GB), Kidney (LI), Spleen (SP) meridians. Changes in these energy meridians can guide the treatment of acupuncture in patients with spinal cord injury.
References
- Craig A, Perry KN, Guest R, Tran Y, Middleton J (2015) Adjustment following chronic spinal cord injury: Determining factors that contrib- ute to social Br J Health Psychol 20: 807-823.
- Kumar R, Lim J, Mekary RA, Rattani A, Dewan MC, et al. (2018) Traumatic Spinal Injury: Global Epidemiology and Worldwide Vol- World Neurosurg 113: 345-363.
- Molina B, Segura A, Serrano JP, Alonso FJ, Molina L, et al. (2018) Cognitive performance of people with traumatic spinal cord injury: A cross-sectional study comparing people with subacute and chronic Spinal Cord 56: 796-805.
- Grauwmeijer E, Heijenbrok-Kal MH, Peppel LD, Hartjes CJ, Haits- ma IK, et al. (2018) Cognition, Health-Related Quality of Life, and Depression Ten Years after Moderate to Severe Traumatic Brain Injury: A Prospective Cohort J Neurotrauma 35: 1543-1551.
- International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI). Version of Disponível em: http://www. asia-spinalinjury.org/elearning/ISNCSCI. Access: 14/12/2019.
- Awad A, Levi R, Waller M, Westling G, Lindgren L, et (2020) Pre- served somatosensory conduction in complete spinal cord injury: Discomplete SCI. Clin Neurophysiol 131: 1059-1067.
- Silvério-Lopes S, da Mota MPG (2018) Influence of acupuncture on the pain perception threshold of muscles submitted to repetitive Br J Pain 1: 207-211.
- Cavalca AMB, Gomes C, Nogueira DA, Rossi-Junior WC, Almeida MSA (2019) The effect of acupuncture on exam anxiety in medical students: A randomized crossover study. Revista Internacional de Acupuntura 13: 43-48.
- Wang L-H, Huang W, Wei D, Ding D-G, Liu Y-R, et al. (2019) Mechanisms of Acupuncture Therapy for Simple Obesity: An Ev- idence-Based Review of Clinical and Animal Studies on Simple Evid Based Complement Alternat Med 579638: 1-12.
- Motlagh FE, Ibrahim F, Rashid RA, Seghatoleslam T, Habil H (2016) Acupuncture therapy for drug Chin Med 11: 1-20.
- Jin BX, Jin LL, Jin G-Y (2019) The anti-inflammatory effect of acu- puncture and its significance in analgesia. World Journal of Acu- puncture - Moxibustion 29: 1-6.
- Tang Y, Yin H-Y, Liu J, Rubini P, Illes P (2019) P2X receptors and acupuncture Brain Research Bulletin 151: 144-152.
- Xu Y, Cai X, Qu S, Zhanga J, Zhang Z (2020) Madopar combined with acupuncture improves motor and non-motor symptoms in Par- kinson’s disease patients: A multicenter randomized controlled trial. European Journal of Integrative Medicine 34:101049.
- Xiao X, Zheng Q, Shi Y, Zhang L, Zhao L, et (2019) Association of Patients’ Characteristics with Acupuncture Treatment Outcomes in Treating Bell’s Palsy: Results from a Randomised Controlled Trial. Evidence-Based Complementary and Alternative Medicine 607348.
- Chang J-S, Liu H-P, Lin W-Y (2016) Acupuncture at SP6 Point in Lower Extremities Improved Patients’ Insomnia, Which Was Also Shown Through Ryodoraku Electrical Acupunct Electrother Res 41: 79-93.
- Smith E, Fitzpatrick P, Lyons F, Morris A, Synnott K (2019) Pro- spective epidemiological update on traumatic spinal cord injury in Spinal Cord Ser Cases 5: 9.
- Kriz J, Kulakovska M, Davidova H, Silova M, Kobesova A (2017) Incidence of acute spinal cord injury in the Czech Republic: a pro- spective epidemiological study 2006-2015. Spinal Cord 55: 870-874.
- Silva BCG, Kamakami LS, Silvério-Lopes S (2014) Energetic profile for electrodiagnostic Ryodoraku acupuncture in patients with Par- kinson´s Journal Integrative Medicine 12: 316.
- The Editors of Encyclopaedia Britannica. Bioelectricity .Publisher Encyclopædia Britannica Inc. November 20, 2018 https://www.bri- com/science/bioelectricity. Access date February 19, 2020.
- Jingjing X, Fan Y, Danhong H, Zhenhai W, Yuankai H, et al. (2018) Low impedance nature of 12 acupoints on the limbs, and the unex- pected dependence on limb J Tradit Chin Med 38: 287-298.
- Ahn AC, Park M, Shaw JA, McManus CA, Kaptchuk TJ, et (2010) Electrical Impedance of Acupuncture Meridians: The Relevance of Subcutaneous Collagenous Bands. PLoS One 5: 11907.
- Di Vincenzo O, Marra M, Scalfi L (2019) Bioelectrical impedance phase angle in sport: A systematic J Int Soc Sports Nutr 16: 1-11.
- Chandrasekaran S, Davis J, Bersch I, Goldberg G, Gorgey AS (2020) Electrical stimulation and denervated muscles after spinal cord Neural Regen Res 15: 1397-1407.
Citation: Silvério-Lopes S, Silva TLD (2020) Energy Profile with Ryodoraku Electro- diagnosis of Acupuncture in Patients with Spinal Cord Injury. J Acupun Tradit Med 3: 008.
Copyright: © 2020 Silvério-Lopes S, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.