*Corresponding Author:
Begoña Torres-Gallardo,
Human Anatomy Unit, Medicine Faculty, University of Barcelona, c/Casanov, 143, 08036 Barcelona, Spain
Email: btorres@ub.edu
Abstract
Ultrasound scan is an image instrument that allows the assessment of diaphragmatic function and it does not have any side effects for patients. We have not found any literature about the use of M-mode ultrasonography to assess the diaphragmatic movement while singing. For this reason, in this paper we intend to assess this movement in two singers (soprano and contralto) after singing a high note and a low one. The diaphragmatic rise, measured as an angle of inclination, was smaller in the high notes than in the low ones in both singers an in all measurements taken.
We consider that the study of diaphragmatic movement by using M-mode ultrasonography can be a study method of the behavior of this muscle while singing. This method, in the future, could be applied to the study of obstructive respiratory pathologies.
Keywords
Diaphragm; Diaphragmatic motion; Singing voice; Ultrasound image
Introduction
M-mode ultrasonography (Motion mode) is a version of the more common mode 2D (also known as B-mode or two-dimensional mode) in which just one ultrasound beam is used. In the M-mode images are obtained unidimensional, in motion and throughout time. The thin ultrasonic beam causes echoes that are identified as hyperechogenic spotsof different depths. These spots draw a line that is represented on the monitor in a continuous way and moves forward towards the right. This allows us to accurately follow the displacements of the structure (changes in depth) throughout the time interval, and for this reason it is very frequently used in echocardiography [1-4].
M-mode has been used by different researchers for the analysis of diaphragmatic motions in healthy individuals [5] and for the assessment of diaphragmatic paralysis in pediatric patients [6-8] and adults [9,10].
In the analysis of the curve in M-mode the inhalation and exhalation times, as well as the cm of diaphragmatic displacement [11] are obtained. We suggest that this examination could be interesting in order to assess the behavior of this diaphragm during the singing maneuvers and yet we have not found any article evaluating this in the specialized literature. For this purpose, the aim of our preliminary study was assessing this behavior in singers during the vocalization of a low and a high note.
Methods
In this initial analysis we have included two professional singers with more than 15 years experience, a soprano and a contralto. Both singers belong to the same singing school and therefore they have been trained according to the same body work. They were asked to sing a high note and a low one. The notes to be sung were chosen by the singing instructor member of the research team, so that they presented a similar level of difficulty for both volunteers. The soprano sang a low note, F3, and a high note, B4, whereas the contralto sang an A2 and a F4.
We used a portable ultrasound scanner (M. Turbo, Sonosite, Bothell, USA). For the 2D ultrasound examination we used a convex 2-5 MHz probe (C60x, Sonosite, Bothell, WA, USA) which was placed in the right hypochondrium window and we could observe in all cases the diaphragmatic cupola as a hyperechogenic line (Figure 1). For the M-mode ultrasoundwe used a sectorial transducer (1-5 MHz) in abdominal preset (P21x, Sonosite, Bothell, USA). The transducer was placed below the breastbone (in the right epigastrium-hypocondrium); towards the right diaphragmatic cupola. Once the diaphragmatic line and the vision of its cupola in 2D had been obtained, the line of the M mode was placed on the image of the cupola and the rise of the diaphragmatic line during the singing was determined. The M-mode image obtained was saved in the system. The diaphragmatic line slope (expressed in inclination degrees) was measured with the public domain software program Image J.
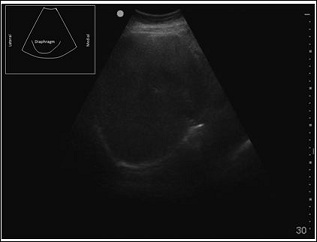
Figure 1: 2D image with the placing of the convex echo sounder in the right hypochondrium. The relevant diaphragmatic line can be clearly seen.
Results
The ultrasound examination was carried out throughout the whole vocalization, and in all cases the displacement of the diaphragmatic cupola from its lowest position (inhalation position) up to its highest position (rest position) could be observed (Figure 2).
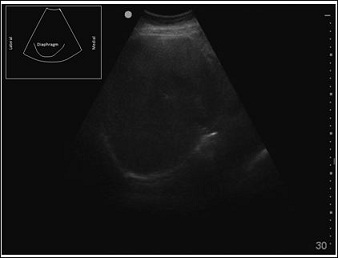
Figure 2: Image of the diaphragmatic movement observed in the 2D mode throughout time. A: inhalation; B: rest.
By means of a 2D ultrasound image we could see that during the production of the low sound in both singers the diaphragm returned accompanying the sound from the beginning of the vocalization. Contrary to this, in the case of the high note the diaphragm didn’t gradually displace accompanying the sound but rather stayed in a tight position and slowly rose until the end of the emission.
In order to objectively measure the diaphragmatic excursion we applied the M-mode ultrasound. By applying this technique to the study of the diaphragmatic motion during the vocalization we have observed, for both singers and in the different trials carried out, that when producing a low note the line drawn by the diaphragmatic excursion shows a greater slope (Figure 3) than that obtained in the case of a high note (Figure 4). This indicates that in the case of the low note the diaphragm rises quicker than in the case of the high one where it remains in a more stableposition throughout the vocalization, which coincides with the results seen in the case of the 2D ultrasound.
Discussion
By means of an M-mode ultrasonography we have been able to observe that for each one of the singers the diaphragm returns more slowly during the production of the high note than during the production of the low one. This behavior of the diaphragm can be explained according to the ideal gases law: P · V = n · R · T (applicable in this case just in an estimated way since air is not an ideal gas). P, V, n and T are four variables, pressure, volume, quantity of gas in moles (a mass unit) and temperature, respectively. When singing a low or a high note we shall only play with three of these variables, since we can consider Temperature (T) to be constant. In the equation R is also a constant, the ideal gases constant.Therefore we obtain the following equation: P · V / n = R · T = constant.
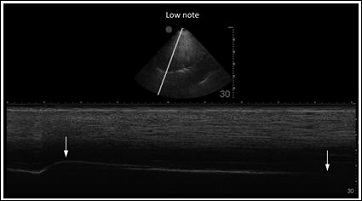
Figure 3: Contralto low note (A2). The diaphragmatic rise is seen as an inclined hyperechogenic line. Inclination angle: 2.84o. Arrows indicate the beginning and the end of the vocalization.In the upper part of the figure the 2D ultrasound imageis shown, where the diaphragmatic cupola, shaped as a curve hyperechogenic line, and the axis that intersects with it and on which its movement along time has been registered can be observed.
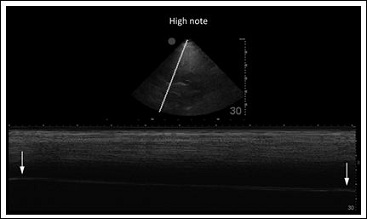
Figure 4: Contralto high note (F4). The diaphragmatic rise is seen as an inclined hyperechogenic line. Inclination angle: 2.06o. Arrows indicate the beginning and the end of the vocalization. In the upper part of the figure the 2D ultrasound image is shown, where the diaphragmatic cupola, shaped as a curve hyperechogenic line, and the axis that intersects with it and on which its movement along time has been registered can be observed.
The vocal folds start vibrating due to the pressure exerted on them by the exhaled air. When this pressure (subglottal pressure) is greater than that of thevocal folds, these later ones are forced to separate from one another and air passes very quickly between them causing a sharp pressure fall in the glottal cleft. This effect, known as the Bernoulli Effect, together with the elasticity of vocal folds, makes the folds come close and the glottal cleft closes.This phenomenon is produced in a quick and repeated way determining the vibration of vocal folds and, therefore, the production of the voice. In the case of a high notethe closure pressure is greater than that in the case of a low note, and therefore we shall need to exert a greater exhalation pressure in the production of a high note than in that of a low one (Torres, 2014).
Whenever we produce a high-pitched sound we need a high pulmonary Pressure (P) in order to make vocal folds vibrate, but the loss of gas (n) is very small since just very little air goes out although at a great speed (that is why a high-pitched sound is produced). And so, since the variation of n is very small, if we return to the equation P · V / n = constant, we see that is virtually not necessary to change the pulmonary Volume (V) in order to keep the necessary pressure to make the folds vibrate, and this makes it possible for us to keep the diaphragm almost still (as we can see in the ultrasound images) while we emit the sound. Only at the end, when we no longer have enough air (n is evidently reduced) we shall need to diminish the volume in order to have enough pressure (we see the diaphragm return at the end of the registry) until we cannot exert any more pressure and the emission ends.
In a low-pitched sound the tension of the vocal chords is low and the necessary pressure to separate the folds shall be less than in the previous case. When this pressure manages to separate the folds, the air flows at a low speed between them (that is why a low-pitched sound is produced). It is worth highlighting that in order to generate this low-pitched sound the vocal folds are separated longer than in the case of a high-pitched sound and that, therefore, the amount of lost air is bigger. This way the n diminishes more quicklyand we need to reduce the pulmonary Volume (V) in order to keep the Pressure (P) on the vocal folds. This explains that the diaphragm goes up and up in a constant manner accompanying the sound during the low-pitched note as we have observed.
Our preliminary results in two singers suggest that the M-mode ultrasound can be applied in a reproducible way for the study of diaphragmatic excursion. It allows, for each individual, to express in an objective way the movement of this muscle during the different vocalizations. We believe that this study can be extrapolated to choral groups by means of portable ultrasound scanners, which allow carrying out the examinations in the rehearsal rooms. Since it is a non-invasive safe technique, it can be used both in adult and infant singers.
The study of the diaphragm’s behavior in pathologic procedures, such as chronic obstructive condition and bronchial asthma, has been used as a prognosis index [12,13]. That is why we think that the presented examination could have clinical interest in the future.
Conclusion
Our preliminary study has limitations. In the first place, we must analyze series of cases in order to establish the soundness of our find- ings. In the second place, we must clearly define the position of the echo sounder during the exploration in order to make sure that our study can be reproduced with general population.
We believe that the analysis of the diaphragm’s displacement in ac- tive exhalation by means of M-mode can be used in the future for the examination of singers (for their teaching or assessment), and it could also be of interest for pulmonary pathological procedures, especially for obstructive pathologies.
References
- Díez N (1992) Principios básicos de la ecografía. Clínica veterinaria de pequeños animales 12: 138-147.
- Balius R, Sala X, Álvarez G, Jiménez F (2007) Ecografíamusculoesquelética. Badalona: Paidotribo.
- Schmidt G (2008) Ecografía: De la imagen al diagnóstico. Madrid: Editorial Médica panamericana 484.
- Kurjak A, Chervenak FA (2009) Donald School. Ecografia en Obstetricia y Ginecologia (2th edn). Madrid: Ed Médica Panamericana 1010.
- Testa A, Soldati G, Giannuzzi R, Berardi S, Portale G, et (2011) Ultrasound M-mode assessment of diaphragmatic kinetics by anterior transverse scan- ning in healthy subjects. Ultrasound Med Biol 37: 44-52.
- Urvoas E, Pariente D, Fausser C, Lipsich J, Taleb R, et al. (1994) Diaphrag- matic paralysis in children: diagnosis by TM-mode ultrasound. Pediatr Radiol 24: 564-568.
- Riccabona M, Sorantin E, Ring E (1998) Application of M-mode sonography to functional evaluation in pediatric Eur Radiol 8: 1457-1461.
- Epelman M, Navarro OM, Daneman A, Miller SF (2005) M-mode sonography of diaphragmatic motion: description of technique and experience in 278 pe- diatric Pediatr Radiol 35: 661-667.
- Lloyd T, Tang YM, Benson MD, King S (2006) Diaphragmatic paralysis: the use of M mode ultrasound for diagnosis in Spinal Cord 44: 505-508.
- Kim SH, Na S, Choi JS, Na SH, Shin S, et al. (2010) An evaluation of dia- phragmatic movement by M-mode sonography as a predictor of pulmonary dysfunction after upper abdominal Anesth Analg 110: 1349-1354.
- Yamaguti WP, Paulin E, Salge JM, Chammas MC, Cukier A, et (2009). Dia- phragmatic dysfunction and mortality in patients with COPD. J Bras Pneumol 35: 1174-1181.
- Ayoub J, Cohendy R, Dauzat M, Targhetta R, De la Coussaye JE, et (1997) Non-invasive quantification of diaphragm kinetics using m-mode sonography. Can J Anaesth 44: 739-744.
- Hellebrandová L, Chlumský J, Vostatek P, Novák D, Rýznarová Z, et al. (2016) Airflow limitation is accompanied by diaphragm dysfunction. Physiol Res 65: 469-479.
Citation:Torres-Gallardo B, Sala-Blanch X, Gimeno-Aragón E, Prats-Galino A (2017) Diaphragmatic Excursion Studied by M-Mode Ultrasonography in Singers. A Preliminary Study. J Case Repo Imag 1: 001.
Copyright: © 2017 Torres-Gallardo B, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
