*Corresponding Author:
Arghya Bandyopadhyay,
Department of Pathology, Burdwan Medical College, The West Bengal University of Health Sciences, Burdwan, West Bengal
E-mail: drarghyabanerjee@yahoo.com
Abstract
Previously several cases of adrenal pseudocysts were reported associated with both benign and malignant tumours. To best of our knowledge, we are reporting the first case of adrenal lipoma with pseudocyst formation possibly due to fat necrosis. The patient presented with a large fat density lesion arising from left adrenal gland. Ultrasonography guided fine needle aspiration smears of the lesion showed clusters of mature adipocytes in a background of acellular, lamellated necrotic fat with foreign body type of giant cells surrounding them. The necrotic fat was misinterpreted as keratin in cytology and the tumour was misdiagnosed as adrenal cystic teratoma. Ultimately the histopathology confirmed the fat necrosis within adrenal lipoma. Here we have discussed the radiological, cytological and histopathological feature of that rare tumour. Awareness of such entity in adrenal gland will improve the diagnostic accuracy of lipomatous adrenal lesions.
Keywords
Adrenal lipoma; Cytology; Fat necrosis; Pseudocyst
Introduction
The adrenal glands are paired retroperitoneal endocrine organs situated within the confines of the Gerota’s fascia in the perirenal fat. Primary adrenal tumours encountered in clinical practice are often functioning tumours, such as adrenal cortical adenomas or pheochromocytomas [1]. While non-functional adrenal tumours are uncommon lesions; one of these is adrenal lipoma [2]. Cystic adrenal lesions are also uncommon and can be classified as pseudocysts, endothelial cyst, epithelial cyst and parasitic cyst [3,4]. Although pseudocysts are the most common clinically recognized adrenal cyst yet there has been no report of pseudocyst formation in relation to adrenal lipoma [3]. Here we report the case of adrenal lipoma with pseudocyst formation due to extensive fat necrosis that was misdiagnosed in cytology smears as cystic teratoma.
Case report
A 48 year old male patient presented with pain and dragging sensation in the left side of abdomen. The pain was of moderate intensity and non-radiating. There was no history of fever, nausea, vomiting or any symptoms related to the lower urinary tract. The regional physical examination revealed bulging in the left hypochondrium. All the routine laboratory tests related to blood were within normal range.
Computed Tomography (CT) Scan of whole abdomen (with both oral and intravenous contrast) showed a large fat density lesion arising from left adrenal gland measuring 12 cm X 8 cm. There was enhancing solid component at the peripheral aspect with areas of cystic change. The lesion had displaced the pancreatic body and tail anteriorly and left kidney inferiorly. The radiological differentials were adrenal dermoid and complex lipomatous lesion of adrenal gland. (Figure 1) He was referred to the department of Pathology for ultrasonography guided Fine Needle Aspiration (FNA) of the lesion. Smears were prepared with gentle pressure and stained with Papanicolaou (Pap) and May-Grünwald-Giemsa (MGG) stains. The stained smears showed clusters of mature adipocytes in a background of acellular, lamellated debris resembling keratin with foreign body type of giant cells surrounding them. Few chronic inflammatory cells and occasional cyst macrophages were also seen. The acellular debris was thought to be keratin with giant cell reaction against them. (Figures 2 & 3) Thus keeping in mind the adipocytes and keratin material a provisional diagnosis of cystic adrenal teratoma was given. The patient was planned for surgery and the tumour was removed. The postoperative period was uneventful. On gross examination the tissue was mostly yellow in color with brownish areas and an area resembling a cyst wall. Histologic examinations of the lesion revealed thinned adrenal cortical tissue attached to which were lobules of mature adipose tissue. Extensive areas of degenerated and necrotic fat were present forming a pseudocyst with distinctive lipomembranous changes. The wall of the pseudocyst showed necrotic adipocytes, foreign body type of giant cells, foamy macrophages and chronic inflammatory cells (Figure 4). The lipid membrane was found to be weakly Periodic Acid Schiff (PAS) positive diastase resistant (Figure 5). However no haematopoietic elements were evident despite of thorough sampling.
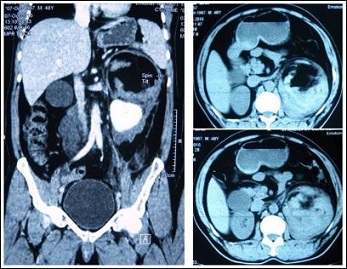
Figure 1: CT scan of abdomen with contrast sowing a large fat density lesion arising from left adrenal, which has inhomogeneously enhancing solid compartment at the peripheral aspect
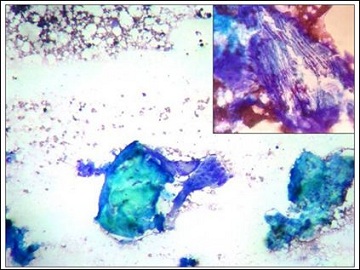
Figure 2: Cytology smear showing necrotic fat as amorphous calcified lamellated debris with foreign body giant cell reaction in a fatty background. (MGG stain, Magnification 100X); Inset: Higher power view of necrotic fat showing lamellated membrane like appearance. (MGG stains, Magnification 400X).

Figure 3: Cytology smear showing necrotic fat with foreign body giant cell reaction. (Papanicolaou stains, Magnification 400X).
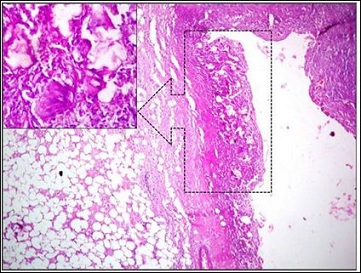
Figure 4: Histopathology section showing lipoma with pseudocyst formation. There is dense fibrosis in the wall of the cyst with presence of necrotic fat, chronic inflammatory cells, giant cells, foamy and hemosiderin laden macrophages (H & E stain, Magnification 40X) Inset: Necrotic fat and foreign body giant cells present in the wall of the pseudocyst. (H & E stains, Magnification 400X).
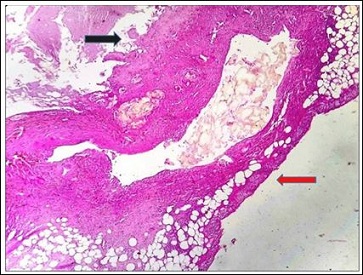
Figure 5: Histopathology section from the fibrotic wall of the pseudocyst showing necrotic fat which is membrane like and showing weak PAS positivity. The black arrow is showing luminal side of the cyst and the red arrow is showing thin rim of adrenal cortex. (PAS stains, Magnification 40X).
Our diagnosis was revised and a new diagnosis of adrenal lipoma with extensive fat necrosis and pseudocyst formation was given. The FNA slides were reviewed. The patient is now recovering and is under follow-up.
Discussion
Adrenal lipomas are very rare lesions. Lam and Lo found 4.8% of the adrenal lipomatous tumours in the 30 year period, of which 0.7% were adrenal lipomas [5]. Although the lesions are asymptomatic in the early stages they are increasingly reported nowadays due to better imaging techniques. The pathogenesis of adrenal lipoma is quite uncertain. They possibly originate from metaplastic changes of either stromal cells or adrenal cortical cells. Histologically, they are similar to lipomas elsewhere in the body. These are well-demarcated lesions composed of lobules of mature adipose tissue separated by thin septa. Focal areas of calcification due to degeneration are noted [5]. The occurrence of fat necrosis in lipoma is quite common in breast while it is uncommon in other locations of the body [6]. Few cases have been reported in the subcutaneous tissues [7]. Most of the reported cases in literature of lipoma with fat necrosis were large tumours as in the present case. In view of their large size, the main cause of fat necrosis was attributed to ischemia induced by trauma or tumour enlargement [7]. Cystic degeneration may occur in such tumours resulting in a cavity formation that contain necrotic fatty material surrounded by multinucleated giant cells. In the late stage the development of fibrosis in the wall leads to pseudocyst formation. The degenerated fat may persist for months or years in the cyst surrounded by calcified fibrosis cyst wall [6]. Histologically, certain variants of fat necrosis such as membranous and nodular cystic fat necrosis have been described in the literature. The nodular-cystic fat necrosis can be differentiated from membranous fat necrosis because the entity is diffusing, non-encapsulated with a cystic appearance having a PAS positive membrane as in our case [8].
In the present case the acellular, lamellated calcified necrotic fatty material with giant cells around them were mistaken for keratin debris and an erroneous diagnosis of cystic teratoma was given. In cytology smear keratin appears more homogeneous and dense, and stained orange, green, blue green or blue depending on staining agents. Whereas calcified fat necrosis is stained purple. In difficult cases, polarized microscopy may be helpful to distinguish between keratin and calcified fatty material. A similar case of lipomembranous fat necrosis in the subcutaneous tissue was misinterpreted as fragments of Echinococcus parasitic cyst wall by Amarapurkar et al [9]. Another finding that was a cause of our error was the presence of a cyst in the lesion as reported by the CT scan examination. There are reported cases of adrenal cystic teratoma that were in turn mistaken as lipomatous lesion by radiology [10]. The pathogenesis of adrenal pseudocyst is mostly believed to be due to organization of a previous traumatic hematoma or a toxic or infectious process or less commonly hemorrhage in an adrenal tumor [3]. Unusual variants of adrenal pseudocyst have been reported, including those with intracystic fat, myelolipomatous metaplasia, metastatic carcinoma and that with features of a dermoid cyst [1-5]. But there has been no reported case of pseudocyst associated with adrenal lipoma. The surrounding necrotic adipocytes and giant cells in the fibrotic wall of the cyst suggest that extensive fat necrosis could have resulted into the pseudocyst formation in the present case.
Conclusion
We thus report a case that is first of its kind, in which both fat ne- crosis and pseudocyst formation occurred in a large adrenal lipoma. Awareness of such entity in adrenal gland will improve the diagnostic accuracy of FNA smears of lipomatous adrenal lesions.
References
- Lam KY (1992) Adrenal tumours in Chinese. Virchows Arch A Pathol Anat Histopathol 421: 13-16.
- Avinoach I, Robinson CR, Avinoah E, Peiser J (1989) Adrenal lipoma: A rare tumour of the adrenal Histopathology 15: 195-196.
- Abershause GA, Goldstein RB, Abeshouse BS (1959) Adrenal cysts: review of the literature and report of three J Urol 81: 711-719.
- Ellis FS, Dawe CJ, Clagett OT (1952) Cysts of the adrenal glands. Ann Surg 136: 217-227.
- Lam KY, Lo CY (2001) Adrenal lipomatous tumours: a 30 year clinicopathological experience at a single J Clin Pathol 54: 707-712.
- Taboada JL, Stephens TW, Krishnamurthy S, Brandt KR, Whitman GJ (2009) The many faces of fat necrosis in the Am J Roentgenol 192: 815-825.
- Nakamura Y, Fujisawa Y, Obara S, Saito A, Nakamura Y, et al., (2013) Giant Lipoma with Fat Necrosis of the Back Mimicking Atypical Lipomatous Tumor in MRI Findings. J Clin Exp Dermatol Res 6:013.
- Ramdial PK, Madaree A, Singh B (1997) Membranous fat necrosis in lipo Am J Surg Pathol 21: 841-846.
- Kavishwar VS, Rupani AB, Amarapurkar AD, Anchinmane V (2008) Diagnostic problems in fine needle aspiration cytology of fat necrosis within a subcutaneous J Cytol 25: 150-152.
- Lam KY, Lo CY (1999) Teratoma in the region of adrenal gland: a unique entity masquerading as lipomatous adrenal tumor. Surgery 126:90-94.
Citation: Roy S, Bandyopadhyay A, Boler AK, Bose K, Nag S (2016) Cytological Findings of Adrenal Lipoma with Extensive Fat Necrosis and Pseudocyst Formation. J Cytol Hisitol 1: 002.
Copyright: © 2016 Roy S, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
