*Corresponding Author:
Raphaella AML,
Anesthesiologist, Coordinator of the Olinda School of Medicine, Assistant Professor at the Federal University of Per- nambuco and at the University of Pernambuco, Recife, Pernambuco, Brazil
Tel: +55 8130115454
Email: raphaella.fernandes00@gmail.com
Abstract
Study objective: Tracheal intubation is a common medical procedure, with one of its indications being to protect the airways of patients at risk of pulmonary aspiration of gastric contents. Sellick’s maneuver consists of compressing the cricoid cartilage against the esophagus at a force of 30 to 40 Newtons (N). The maneuver acts as prevention against possible respiratory complications secondary to pulmonary aspiration. Factors associated with the effectiveness of the maneuver include the professional’s ability to locate the structures and the force applied, both of which affect the final outcome. This study aimed to evaluate both the force used in Sellick’s maneuver on a human airway model and whether pressure was applied at the correct location. Additionally, a possible correlation was analyzed between appropriate/inadequate performance and the professional category of the volunteers, as well as their years of experience.
Design: A cross-sectional study.
Setting: A teaching hospital and a public general hospital.
Participants: Resident anesthesiologists and anesthesiologists working at the teaching hospital, Federal University of Pernambuco, and at the Barão de Lucena Hospital.
Interventions: Participants were asked to perform Sellick’s maneuver three times on an airway model and were blinded to results.
Measurements: After disclosure of the results, participants who failed to perform the maneuver correctly underwent a brief training.
Main results: Fifty medical residents participating in the three-year residency program in anesthesiology and 33 anesthesiologists with varying years of experience were evaluated. According to a questionnaire, 45.8% of participants performed the maneuver regularly and 86.7% worked in emergency departments. Nevertheless, mean force applied ranged from 27.22 to 27.76 N and the rate of inadequate performance ranged from 73.5% to 75.9%. No significant association was found between performance and professional category or years of experience.
Conclusion: Most of the professionals participating in this study did not perform Sellick’s maneuver appropriately.
Keywords
Anesthesiology; Pressure; Sellick’s maneuver; Tracheal intubation
Introduction
Managing the airways is one of the principal challenges faced by healthcare professionals. Of the different procedures used, tracheal intubation merits particular mention as it is frequently indicated and used in anesthesiology. Multiple interventions are generally used to avoid complications and to maintain the patency of the upper airway and spontaneous ventilation; therefore, adequate knowledge of the pertinent anatomy and of how each maneuver should ideally be performed within this management approach is vital.
In the many cases of patients who have not fasted appropriately or in those with slow gastric emptying, the likelihood of regurgitation and aspiration of the gastric contents to the respiratory system during anesthesia [1-3], with consequent pulmonary complications [4], has to be reduced.
Monro first described compression of the cricoid cartilage in 1774; however, it only became popular in 1961 when the anesthesiologist Brian Sellick described it as a means of preventing gastric aspiration following induction of anesthesia [5-7] during rapid sequence intubation [1,3,8-10]. Sellick’s maneuver is a procedure that consists of applying pressure to the cricoid cartilage against the sixth cervical vertebra in order to compress the esophagus and prevent regurgitation [7,11,12].
Although the level of evidence is low and there are disadvantages associated with Sellick’s maneuver [13,14], it is routinely used by medical and paramedical teams [9,10]. The maneuver is claimed to be a simple, inexpensive technique that delivers the desired outcome as long as the professional performing it is capable of accurately locating the cricoid cartilage and applying the correct amount of force [5,9,13,15]. From a legal point of view, the procedure is understood as an auxiliary measure to reduce the risk of pulmonary aspiration [8].
In this respect, following loss of consciousness and with the application of force of 30 to 40 Newtons (N) [4,9-11,15,16] on the cricoid cartilage, the likelihood that the maneuver will be successful increases, even in situations in which there is an increase in gastric pressure [2]. Some studies, however, have detected the use of pressure levels below that recommended in the literature when different professionals performing Sellick’s maneuver were evaluated [9,15,17].
The objectives of the present study were to determine the force in N applied during Sellick’s maneuver, to evaluate participants’ ability to locate the correct anatomical structure during performance of the maneuver, and to correlate these variables with the time of practical experience in anesthesiology.
Materials and Methods
This was a cross-sectional study conducted in the state of Pernambuco, Brazil in which 50 medical residents in anesthesiology and 33 anesthesiologists working at the teaching hospital of the Federal University of Pernambuco and at the Barão de Lucena hospital were evaluated. The internal review board of the Federal University of Pernambuco approved the study protocol.
After signing the informed consent form, the participants completed a short demographic questionnaire and were shown a human airway model placed on a high precision scale. The airway model was developed by the researchers. Each participant was then asked to point out the exact location of the structure at which Sellick’s maneuver should be performed and to apply pressure onto this structure three times. The attempt closest to the recommended guidelines was the value computed for that participant in the study. The participants remained blinded to their results up to the final analysis.
The categorical variables were expressed as absolute distributions and percentages, while means and standard deviations were used for the numerical variable force. Pearson’s chi-square test was used to determine significant differences between the categories evaluated in relation to whether the amount of force used was appropriate or inadequate. When the conditions for the use of Pearson’s chi-square test were not fulfilled, Fisher’s exact test was used.
The margin of error considered in the statistical analysis was 5%. The program used for data entry and analysis was the Statistical Package for the Social Sciences (SPSS), version 17.
Results
The characteristics of the study participants are shown in table 1. Women comprised 54.2% of the sample, with most being medical residents in anesthesiology. Of the anesthesiologists, most had completed their specialization training less than 10 years previously. Overall, 45.8% of the participants reported that they performed the maneuver frequently.

Table 1: Characteristics of the participants in the study sample (n=83).
Table 2 summarizes the participants’ attempts to locate the structure at which Sellick’s maneuver should be performed on the airway model. Although the group of anesthesiologists was less accurate compared to the medical residents, this difference was not statistically significant.
Table 3 shows the amount of force applied at each maneuver and the mean value for the three attempts. The amount of force ranged from 27.22 N to 27.76 N, with a mean of 27.52 N. Variability was not high, with standard deviations being less than half the values of the corresponding means.
Tables 4 and 5 show the amount of force categorized into appropriate or inadequate, taking into consideration each attempt made by the professionals and the mean force exerted at the three attempts. As shown in Table 4, at all their attempts the residents in anesthesiology were more likely than the anesthesiologists to apply an inadequate amount of force.

Table 2: Ability to locate the correct structure at which to perform Sellick’s maneuver, according to professional category.
aPearson’s chi-square test
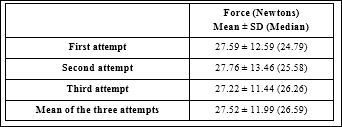
Table 3: Force applied at each attempt to perform Sellick’s maneuver and the mean value for all the attempts.
However, at the established margin of error of 5%, there was no statistically significant difference between the group of residents in anesthesiology and the group of anesthesiologists. The results for the group of residents are detailed in Table 5 as a function of the year of their residency, with the subgroup of second-year residents performing better compared to the other subgroups; however, the percentage of second-year residents applying inadequate force was still greater, although not significantly so, than the percentage of anesthesiologists.
As shown in Table 6, the subgroup of anesthesiologists who completed their specialization less than ten years previously was more successful in applying the appropriate force needed compared to those who completed their specialization more than ten years previously. However, no statistically significant association was found between time since specialization and the force applied at each attempt or the mean force achieved in the three attempts.
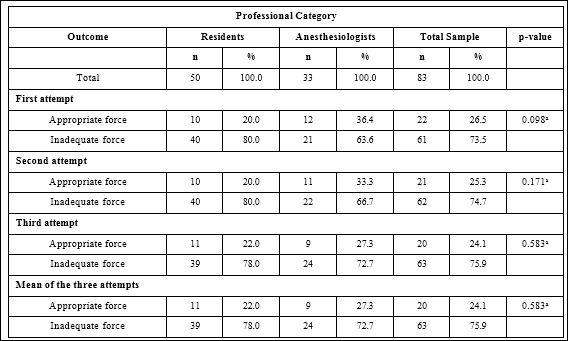
Table 4: Force applied at each attempt to perform Sellick’s maneuver and the mean force applied for the three attempts, classified as appropriate or inadequate, according to professional category.
aPearson’s chi-square test

Table 5: Force applied at each attempt to perform Sellick’s maneuver and the mean applied for the three attempts, classified as appropriate or inadequate, according to professional category and year of residency.
aFisher’s exact test
Discussion
The present study evaluated both the performance of the participants in identifying the location of the cricoid cartilage on the airway model and the amount of force applied for Sellick’s maneuver, and assessed these factors as a function of years of experience.

Table 6: Force applied at each attempt to perform Sellick’s maneuver and the mean at all the attempts, according to time since completing specialization in anesthesiology.
aFisher’s exact test
The residents were better at accurately locating the site of the cricoid cartilage for the maneuver, while the anesthesiologists who had completed specialization less than 10 years previously were better at using the appropriate force to perform cricoid pressure effectively; nevertheless, there was no statistically significant difference between the residents and the more experienced anesthesiologists.
Sellick’s maneuver is recognized by the American College of Emergency Physicians. The procedure is routinely used by anesthesiologists and constitutes routine practice in most European countries [18]. Nevertheless, a recent study conducted in 2013 compared the amount of pressure applied in Sellick’s maneuver by anesthesiologists, general practitioners, residents in clinical medicine and anesthesiology, nurses, nursing aides and physiotherapists, and found that all the different professionals tended to use less pressure than that recommended in the literature [9]. Those findings are similar to those of the present study.
Studies conducted in Australia and in the United States involving physicians and nurses reported accuracy rates of 25% and 26.2%, respectively, for the performance of Sellick’s maneuver on an airway model [15,17]. Those results were also similar to the findings of the present study, with no statistically significant difference being found between the two groups analyzed. This poor rate of accuracy in performing the maneuver, as shown in various studies, could be related to a lack of training [19] following specialization, since residents in anesthesiology already at this stage perform the procedure inadequately.
Using questionnaires, a study conducted in the United States evaluated whether a group consisting of physicians, medical residents and nurses performed Sellick’s maneuver at the correct location [12]. Results showed that 67.4% of the sample accurately located the cricoid cartilage, a percentage that is similar to the 71.1% found in the present study. Another cross-sectional study conducted with paramedics reported that 100% of surgical nurses correctly located the site for the maneuver [16]. The high percentage of accuracy in the group of nurses could be related to the fact that physicians or anesthesiologists are often available to assist this professional category as they perform the maneuver, thus providing support and help when necessary.
In those studies, comparisons were made between different professional classes; however, a study conducted in Brazil involving only anesthesiologists with varying years of experience reported that only 23.1% stated that they knew the correct amount of pressure to be applied in Sellick’s maneuver and, of this percentage, only 3.8% were able to say what the recommended pressure was [20]. Although the present study did not evaluate participants’ prior theoretical knowledge of Sellick’s maneuver, results show that the residents performed better at locating the site of the maneuver, while the anesthesiologists were better at applying the recommended pressure. This may suggest that since the residents are still working in an academic environment, it is easier for them to identify the cricoid cartilage, whereas the anesthesiologists, who have been working in medical practice for longer, may have developed the appropriate psychomotor skills associated with the procedure, bearing in mind the number of times they have performed it in clinical practice. Nevertheless, it is a concern that 36.4% of the anesthesiologists were unable to locate the correct site on the neck at which to perform the maneuver; therefore, consideration should be given to the amount of time devoted by professionals to continued education and training. A study conducted in the Brazilian city of Recife showed that many anesthesiologists report exhausting workloads, resulting in clinical manifestations that include tiredness, somnolence and reduced learning capacity, with little time for study [21].
Furthermore, from the time of specialization onwards, there appear to be gaps in learning and this could have important repercussions including inaccuracies in the performance of the maneuver, which would then fail to protect the patient from pulmonary aspiration and hamper laryngoscopy.
The objective of this study was to draw the attention of anesthesiologists, both those in training and those already qualified, to the importance of continued training in the performance of Sellick’s maneuver, and to provide them with feedback and further supervised practice following data analysis. The importance of this cohort lies in the conclusions of the 2013 systematic review affirming that skill at performing esophageal compression decreases as a function of the number of years since graduation and that the use of simulators would represent an effective training tool [19].
Limitations of the present study include the simplicity of the simulator used and the fact that a high precision rather than a very high precision scale was used to measure force. In addition, no data were collected on participants’ previous theoretical knowledge regarding the correct amount of force to be applied and the correct anatomical structure for Sellick’s maneuver.
In conclusion, the results of the present study show that, irrespective of years of experience or professional category, the professionals evaluated here failed to perform Sellick’s maneuver appropriately, both with respect to being able to locate the relevant anatomical structure and regarding the amount of force to be applied.
Funding Sources
This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.
References
- Taylor RJ, Smurthwaite G, Mehmood I, Kitchen GB, Baker RD (2015) A cricoid cartilage compression device for the accurate and reproducible application of cricoid Anaesthesia 70: 18-25.
- Moro ET, Goulart A (2008) Compression of the cricoid cartilage. Current aspects. Rev Bras Anestesiol 58: 643-650.
- Moro ET, Módolo NSP (2009) Tracheal intubation and the patient with a full stomach. Rev Assoc Med Bras (1992) 55: 201-206
- Yamanaka CS, de Góis AFT, Vieira PCG, Alves JCD, de Oliveira LM, et (2010) Orotracheal intubation: physician’s knowledge as- sessment and clinical practices in intensive care units. Rev Bras Ter Intensiva 22: 103-111.
- Trethewy CE, Burrows JM, Clausen D, Doherty SR (2012) Effec- tiveness of cricoid pressure in preventing gastric aspiration during rapid sequence intubation in the emergency department: Study pro- tocol for a randomised controlled trial. Trials 13: 17.
- Brisson P, Brisson M (2010) Variable application and misapplication of cricoid pressure. J Trauma 69: 1182-1184.
- Bhatia N, Bhagat H, Sen I (2014) Cricoid pressure: Where do we stand? J Anaesthesiol Clin Pharmacol 30: 3-6.
- Beavers RA, Moos DD, Cuddeford JD (2009) Analysis of the appli- cation of cricoid pressure: Implications for the J Perianesth Nurs 24: 92-102.
- Calvache JA, Sandoval MX, Vargas WA (2013) Pressure applied by the healthcare staff on a cricoid cartilage simulator during Sellick’s maneuver in rapid sequence Rev Colomb Anestesiol 41: 261-266.
- Benkhadra M, Lenfant F, Bry J, Astruc K, Trost O, et al. (2009) Cricoid cartilage and esophagus: CT scan study of the dynamic variability of their relative positions. Surg Radiol Anat 31: 537-543.
- Páez JJ, Navarro JR (2010) Controversial issue of cricoid pressure or Sellick maneuver. Rev colomb anestesiol 38: 377-383.
- Nafiu OO, Bradin S, Tremper KK (2009) Knowledge, attitude, and practice regarding cricoid pressure of ED personnel at a large S. teaching hospital. J Emerg Nurs 35: 11-15.
- Rice MJ, Mancuso AA, Gibbs C, Morey TE, Gravenstein N, et al. (2009) Cricoid pressure results in compression of the postcricoid hypopharynx: the esophageal position is irrelevant. Anesth Analg 109: 1546-1552.
- Salem MR, Khorasani A, Saatee S, Crystal GJ, El-Orbany M (2014) Gastric tubes and airway management in patients at risk of aspira- tion: history, current concepts, and proposal of an Anesth Analg 118: 569-579.
- Clark RK, Trethewy CE (2005) Assessment of cricoid pressure ap- plication by emergency department Emerg Med Australas 17: 376-381.
- Black SJ, Carson EM, Doughty A (2012) How Much and Where: Assessment of Knowledge Level of the Application of Cricoid Pres- J Emerg Nurs 38: 370-374.
- Lefave M, Harrell B, Wright M (2016) Analysis of Cricoid Pressure Force and Technique Among Anesthesiologists, Nurse Anesthetists, and Registered Nurses. J Perianesth Nurs 31: 237-244.
- Harris T, Ellis DY, Foster L, Lockey D (2010) Cricoid pressure and laryngeal manipulation in 402 pre-hospital emergency anaesthetics: Essential safety measure or a hindrance to rapid safe intubation? Resuscitation 81: 810-816.
- Johnson RL, Cannon EK, Mantilla CB, Cook DA (2013) Cricoid pressure training using simulation: A systematic review and me- ta-analysis. Br J Anaesth 111: 338-346
- Guirro UBP, Martins CR, Munechika M (2012) Assessment of an- esthesiologists’ rapid sequence induction technique in a university Rev Bras Anestesiol 62: 335-345.
- Calumbi RA, Amorim JA, Maciel CMC, Filho OD, Teles AJF (2010) [Evaluation of the quality of life of anesthesiologists in the city of Recife]. Rev Bras Anestesiol 60: 42-51.
Citation: : de Siqueira JWM, Neto JMS, de Assis ALA, de Oliveira JFG, Tavares WTD, et al. (2020) Cricoid Force during Sellick’s Maneuver on a Human Airway Model as Performed by Anesthesiologists and Resident Anesthesiologists. J Anes Perio Manag 4: 009.
Copyright: © 2020 de Siqueira JWM, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.