*Corresponding Author:
Augustin Mubiayi Mamba,
Department of Psychology, University of Kinshasa, Democratic Republic of Congo
Tel: +243999937195
Email: augmamba@gmail.com, augustinmamba@yahoo.com
Abstract
Improved maternal health remains a major concern of the United Nations in general and of the World Health Organization in particular, which have placed an important place on the Millennium Development Goals (MDGs) as well as in the objectives for Sustainable Development (SDO). Curiously, among the causes of complications of childbirth and pregnancy, the emphasis is more on physiological than psychosocial deaths, whereas in our least developed countries, where the percentage of maternal is mortality, cultural and psychological problems expose women to unwanted pregnancies and psychic traumas that manifest themselves during parturition in the form of eclampsia, haemorrhage and work defects, thus leading the woman and her baby to the risk of death.
In the present work, we have proposed a protocol to help childbirth, inspired by the therapeutic practices of our African cultures. Indeed, our ancestors were able to solve the complications of childbirth by speech. The interview with woman with complications around her life and relationships triggered a kind of catharsis in the latter, the labor of childbirth was normal again and the delivery was normal.
The protocol comprises three components: psychodynamic interview, prophylactic psychoeducation, psychological support.
This protocol is based on the humanistic theories of Carl Rogers and Maslow and the sophrology of Alfonso Caycedo and consists in subjecting the parturient to a relaxation exercise by alternate breaths and haptonomy in a helping relationship to allow communication between the woman and her child who is to be born.
Keywords
Childbirth; Complications; Haptonomy; Parturient; Psychodynamic interview; Psychological support; Relaxation
Introduction
In the Luba-Kasai culture, when the parturient delays in giving birth or presents complications, it is presumed that there is a problem related to the violation of customs. To help her to give birth normally, one needs to talk to her in order to obtain an admission, a confession. This triggered labor and caused the woman to give birth normally. Inspired by this practice, we have developed a protocol that goes beyond violations of customs as the only diagnostic pathway at the base of the complication of childbirth. We assumed that there would be psychosocial problems that would underlie the inhibition or slowness of childbirth and that these inhibitory factors can be unlocked using this protocol, which allows the resumption of childbirth and normal childbirth.
This protocol consists of: (i) a psychodynamic interview that allows, apart from the medical diagnosis, to quickly explore with the parturient her past and experience of the pregnancy; (ii) a psychoeducation on what the parturient should know about her pregnancy and childbirth; (iii) psychological support based on anxiety and stress of the woman.
Definition of the Techniques Used
Psychodynamic interview
Clinical psychology is based on: observation, interview and testing. They are all used by the clinical psychologist during the clinical examination to report to a third party a notice. The clinical attitude calls for the fundamental postulates of clinical psychology: dynamic (from a diachronic point of view) and interactionist (from a synchronic point of view). This refers to the helping relationship. It is this relationship that Carl Rogers [1] calls a permissible and precisely structured relationship, which allows the client or patient to gain an understanding of himself to a degree that makes him able to progress to the light of its new orientation. Any caregiving relationship involves the presence of the caregiver (clinician psychologist, psychiatrist, doctor, nurse or other personnel empowered to provide assistance) and the subject or care receiver (the person in a situation of congruence, help).
Interview is the main instrument available to the clinical psychologist, be it for assessment or therapy. Most of the information comes from the discourse of the particularity invited to make exist the objects, the facts, the situations outside their concrete presence. The word of the subject remains the central element and the interview as space between two or more subjects, makes it possible to say, to invalidate, to listen and to exchange [2].
For their part, Bénoy and Chahraoui [3] emphasize that the interview aims to apprehend and understand the psychological functioning of a subject by focusing on his experience and emphasizing the relationship. It is one of the best ways to access the subjective representations of the subject.
According to Cyrille Bouvet and Abdel Halim Boudoukha [4], the clinical interview is first of all an interview, thus a verbal and nonverbal exchange, generally between two persons: the psychologist and one person, subject, patient or client, sometimes more in couple or family interviews). It is clinical, that is, centered on the psychic life of the subject; the psychologist uses specific techniques to approach the psychic intimacy of the subject (active listening, reformulation, empathy, etc.); it takes place within a specific institutional framework (private practice, hospital, etc.) and is part of specific clinical interventions (support, exploration, assessment, psychotherapy). The quality of the clinical relationship (therapeutic alliance) is at the heart of the clinical interview.
Prophylactic psychoeducation
Psychoeducation, a discipline specializing in prevention and intervention in the field of psychosocial maladjustment, is used in this protocol to prevent or alleviate anxiety and stress caused by women’s experiences. Some women come to the birth already with an idea to undergo caesarean section, of course without imagining the risks that it can sometimes involve [5].
The work of Henri Laborit quoted by Marcel Renou [5] also provides a plausible way of integrating available knowledge about human action. Here are the following assumptions:
- The community is an ecosystem functioning mainly according to sociocultural norms which often favor the development of hierarchies by creating among its members, the relations of power of the dominator to Most technical, economic and political information is thus held by a limited number of individuals. They use it to meet their needs more easily and without always foreseeing the negative consequences that this could entail in general. This status of dominance, acquired or preserved, cultivates stereotyped and rigid relations between individuals and conditions a strong inhibition of creative action among the dominated.
- The individual in difficulty is the one whose adapted action is inhibited or thwarted, and which is limited to stereotyped actions or simple reactions. This fact reduces or hinders the harmonious functioning within and between each of the biological, psychological and socio-cultural The individual, who achieves social difficulties, as is common in the current hierarchical sector, will only achieve a precarious balance. This result, apart from being frustrating at the social level, will ultimately lead to deterioration in the psychological and biological functioning of this individual. What he learns then is the ineffectiveness of his actions, which lead him to a still greater inhibition.
- Stopping or disturbing individual development, caused by inhibition of action, imposes a limit on the growth of the This has consequences for the other members of the community and, by extension, for the development of the community as a whole. The latter, thus limited, will actively contribute to the increase of the difficulties of adaptation among its members, since the latter will not find in their socio-cultural environment the conditions favorable to a creative action.
We are thus led to say as Renou that the biopsychosocial postulate forces us to consider the exchanges between the actors according to a grid where the biological, psychological and social components of the individual are in constant inter-influence. Social exchanges depend on the relationship between the personal cultures of the actors involved within the same structure. Relations of dominators to dominated ones can be established and will have the effect of inhibiting the creative action of some of the dominated actors. This inhibition of action will be an obstacle to their adaptive approach to the environment and will become a source of deviance. The deviance of one or more actors will be a source of tension for the whole structure and will thus threaten its balance.
This intervention requires a willingness to help people in need, interpersonal skills and an ability to communicate with them, have an excellent analytical capacity to understand problems in different environments, To have a good sense of observation in order to identify the weaknesses and strengths of individuals to have a spirit of initiative and to exercise good judgment in order to intervene effectively, to like to work in a team with colleagues Different formations.
Psychological support
As we have pointed out above on the helping relationship, psychological support is understood here as psychological or moral comfort allowing the subject to accept the situation and regain the energy necessary for survival. We were inspired by Alfonso Caycedo’s sophrology of improving well-being in the individual guided by two disciplines: phenomenology at the investigation stage and clinical experimentation for verification. This method, applied to childbirth, presupposes from the clinical and theoretical point of view that childbirth is only an epiphenomenon between pregnancy and maternity.
This pregnancy, like childbirth, like motherhood, is accompanied by conscious and unconscious physical and psychological transformations in women. But these transformations also have repercussions on the family environment. The techniques of the sophrologist must therefore support the delivery of childbirth in a positive way by offering the woman a good acceptance of herself, her femininity and her maternity. While in the other methods we replace the conditioned contraction-pain reflex by a different contraction-respiration reflex, in sophrological state, the woman who gives birth does not flee the contractions, she lives them. We speak of a positive effect [6].
This method proceeds by:
- Relaxation in order to obtain a great relaxation and access to facets buried in We cannot forget the ten benefits of deep breathing evoked by Julie Marchand (2014): detoxify the body, increase oxygen in the blood, decrease stress and anxiety, improve posture, help manage Emotions, strengthen the immune system, improve concentration, sleep, digestion and increase vitality. Yet the parturient is in great need of virtually all of these benefits of deep breathing or relaxation.
- Haptonomy: This recent technique deals with affectivity, or laws governing affective mechanisms especially in interpersonal relaHaptonomy consists in connecting by touch, emotional-psycho-tactile contact. This technique is currently recommended in preparation for birth, in painless delivery.
Methodology
Population and sample
The population of this study is made up of pregnant women received at the Maternity Clinic of Kintambo, Kinshasa, Democratic Republic of Congo, during the period running from 1st April to 30th September 2016. A total of 1,238 women gave birth in this medical institution during the study period. From this population, 101 women with various complications on parturition were treated by the application of our protocol.
Terms and conditions
This protocol is valid in one of the following conditions, apart from the pathologies or malformations declared by the obstetrician:
- Being a pregnant woman at term (between 36 and 42 weeks)
- Present a defect of child labor
- Show signs of psychogenic hypertension
- To manifest an unwarranted fear
- Lack of pushing forces
Methods and techniques
We used the clinical method materialized by three techniques: clinical interview, psychoeducation and supportive psychotherapy.
The clinical interview consisted of creating a climate of trust between the psychologist or the caregiver and the parturient in order to induce the latter to say what disturbs her. The particularity of this interview is that the psychologist or the clinician creates a context (relationship, framework, technique) allowing the subject to express his intimate psychic life with confidence without feeling constrained. This is very important on ethics and deontology aspect.
Psychoeducation has pedagogical, behavioral and psycho-affective dimensions. We have provided the subjects with the necessary information on the psychology of pain, the secret of the pain of childbirth which binds forever, whatever the distance, the mother to her child. The mother should know this mystery in order to accept with joy the pain of childbirth and thus transform it into pleasure. As part of our field experience, we highlighted the pleasure of childbirth in Lingala (one of the four national languages in the DRC): “Kobota elengi and elengi ya kobota = to give birth this is a pleasure”.
Finally with supportive psychotherapy, we used two techniques: relaxation and haptonomy. We asked the parturients, after having listened to them, to make some deep breaths and to touch their bellies regularly where they smell their babies, and talk to them affectionately. During this affectionate contact, the mother can ask her baby to come at the moment or in a suitable time.
All these women where approached a day after or the same day of their arrival at the clinic and the French language and lingala (one of the national language in DRC and common in the capital City Kinshasa) were used. We used statistic analysis and the case study for the results.
Presentation of Results
The results of our research are presented in the tables below which classify women’s birth modes for the general situation and those we followed, provinces of origin and type of births.
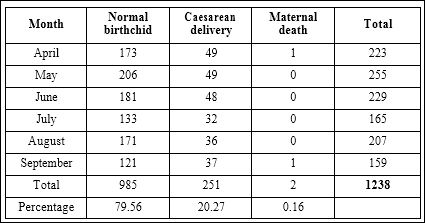
Table 1: Births registered between April and September 2016.

Table 2: Births registered between April and September 2016.

Table 3: Complicated deliveries followed between April and September 2016.
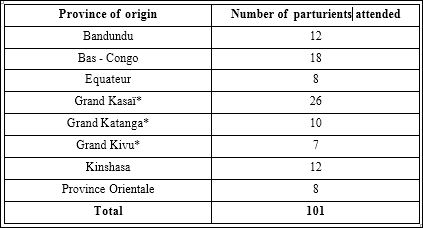
Table 4: Breakdown by origin provinces.
(*)We grouped provinces with the same culture under the prefix “grand”
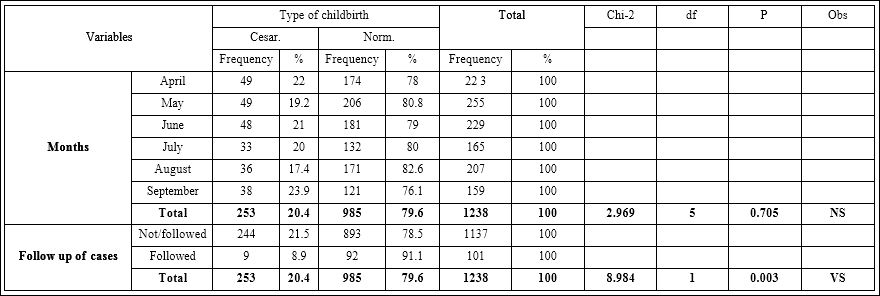
Table 5: Type of childbirth versus independent variables.
At the end of our psychodynamic interview, the following problems were identified as inhibitors or disrupters of labor:
- Pregnancy by rape
- Refusal of the man to recognize his pregnancy
- Fear of the Caesarean section following the death of a sister of the parturient by this way
- Death in utero
- Fear of pain
- Infidelity
- Attempted abortion on several occasions
- Unresolved mourning at the end of the loss of a mother
- Lack of financial means to raise the child
Analysis of the Results
For this analysis, we considered as independent variables the months during which deliveries occurred during our study (April, May, June, July, August, and September) and follow-up of cases (women followed according to our protocol or not), while the dependent variables are the type of childbirth (normal or caesarean) and the situation at birth (alive and / or dead).
The combination and manipulation of data collected according to the methodology explained above will allow us to draw conclusions on the protocol of psychological assistance to delivery that we have set up.
The following table show the crossings between variables and explain how or not there are correlations between them and whether the apparent differences between the frequencies are significant or due to fluctuations in sampling.
Interpretation
Type of childbirth compared to months
The contingency table above, which combines the childbirth frequencies per month with the type of childbirth, allowed us to have a Pearson’s Chi-2 equal to 2.969 with a degree of freedom of 5 and the SPSS program allowed us to obtain an associated probability of 0.705. Since p = 0.705> α = 0.05 / 0.01, it can be deduced that the difference between childbirth type frequencies compared to months is not significant. Therefore, we conclude that months do not affect the type of childbirth. In other words, the fact that a woman gives birth by caesarean, for example, is not due to the month in which she gives birth; which means that the months did not affect the type of childbirth.
Type of childbirth versus case follow-up
Regarding to the association of the independent variable type childbirth with the dependent variable case follow-up , the contingency table gives us a Chi-2 = 8,984 with a degree of freedom of 1. The associated probability is p = 0.003 ≤ α = 0.01 / 0.05. So the difference between the frequencies is very significant. As a result, we conclude that case follow-up, which means applying the protocol of psychological assistance to delivery, has had a very great impact on the type of childbirth or even better in the improvement obtained at delivery. This means that psychological follow-up has been the foundation of little cesarean delivery and many normal deliveries.
Case Study
The case study was a crucial step in the application of the clinical method. It formed the bedrock of our direction for this research. The clinical observation of pregnant women in parturition was done using a notebook and pen as well as a botanical observation consisting in recording all the facts and gestures of the parturient.
The psychodynamic interview allowed us to do the psychology of depth to understand the lived experience of the parturient, its anxieties and its suffering likely to complicate the childbirth. This step was very difficult, especially since we worked in an emergency situation, so the time was not on our side. It was necessary to identify the problem in a very short time and provide for its resolution.
Prophylactic psychoeducation has facilitated a penetration into the psyche of the parturient so that she understands her problem and accepts our approach. It was here that we left the woman in parturition to decide on her fate. At this stage, the tension, the pains, the stress of the parturient and all her anxieties were attenuated.
During the psychological support, the parturient could act at ease and for some of them, the delivery was done without them realizing it that can be called birth without pain, while these pains still existed but converted into pleasures. The haptonomy and the deep breaths were concomitantly used to bring the parturient to spend some moments of relaxation and harmony. This leaves the body to do the work while the psyche was in perfect homeostasis.
The results obtained after the administration of this protocol shows how effective it was, because the initiation or improvement of the delivery work after the follow-up was done between 10 to 30 minutes later, and the delivery took place between 45 minutes to two hours, except for very complicated cases that could last up to six hours.
The case study highlighted the entire procedure used in this research and was greatly admired by the midwives and physicians who participated in our research. Some of them did not fail to say at first that it was magic. But over time, everyone understood the process and there was a good symbiosis.
Some clinical cases
Betty case
Betty is third in her siblings after two boys from a Luba family in Kasai with eight children. She is 36 years old and married to a man with no fixed function. Her father died when Betty was only 10 years old.
Betty is 40 weeks pregnant and has been admitted to the Maternity Hospital since 5:00 pm on a Wednesday for delivery. Upon arrival, the dilatation of his cervix was 3cm. We receive it the next day, a Thursday at 11:17; because the medical staff finds that his work is not progressing.
We began by checking with the medical staff and from her consultation sheet and the partograph, whether Betty had known or reported antecedents. Thus, we engaged in our exercise of help with our protocol.
Psychodynamic interview: Our interview was intended to explore Betty’s life since her childhood, the story of her maturation and her pregnancy, in order to find the traumas buried in her unconscious, the psychogenic situations of her life that could be at the root of the blockage from his work.
Having gained her trust, Betty will reveal to us that in her father’s family, there are many wizards who say that if a woman in the family gets married, she should not give birth and if she dares to get pregnant she will die at delivery.
When Betty got married, her husband lost his job a few days later, and the social life in their conjugal roof had become untenable. She had to make two miscarriages and with this third pregnancy that came to an end, she was very afraid either to repeat another miscarriage or to die as the wizards of her father’s family promise.
We recommended him to take a few deep breaths before continuing with our second stage of the protocol, namely prophylactic psycho education
Prophylactic Psychoeducation: We seized the problem that disturbed Betty in her psycho-emotional life: belief in the witchcraft of her father’s family with the two previous miscarriages and the probable death that would await her at birth as she believes herself guilty of having violated the motto of his family. So the death of her father affected her a lot, leaving behind a badly resolved Oedipus complex that makes her live in insecurity.
Pedagogically, we explained to our parturient that each case was unique, that there are no links between her miscarriages and her current pregnancy. Then, we convinced her that she was going to give birth in good conditions because she was out of her natural environment where she could see the wizards everywhere.
Psychologically, we asked Betty to remove from her head (her psyche) all the negative thoughts about death that would haunt her and all forms of anxiety.
Behaviorally, we recommended that Betty understand that her positive attitude is a very effective way to reactivate her labor and give her the joy of becoming a mother. What we called “Elengi ya kobota”, in Lingala. This finally allowed us to engage in the last phase of our protocol which is psychological support.
Psychological support: This phase consisted of asking Betty to talk with her baby by touching her belly where she feels it and feeling it gently, and giving her beautiful words silently or loudly (haptonomy).
Betty had to tell her baby to go out immediately because she was ready to receive him.
So we told Betty to practice deep breaths whenever she felt fear, anxiety, or any negative thought coming through her head.
Result: After administering Betty this protocol, it took thirty minutes for the contractions to resume and the dilation accelerated so much so that at 15:20, Betty gave birth to her beautiful little boy of 3,500 kg without much suffering.
It should be noted here that Betty, in her head, expected to have a daughter, which wanted to put her in a state of annoyance. Our role was to support her and make her understand that the baby was always a beautiful gift carrying joy and happiness whatever her sex. She had an interest in showing all the affectivity to her baby so that he could grow in balance.
With Betty, our job was to make him stand out or make him confess to this problem that was blocking the birth of his baby: it is the fear of death because of the sorcery perceived in his family, triggering of normal work childbirth (catharsis)
Bokoy case
Bokoy is a young lady of 26 years old. She is the fourth of five siblings, married to an official of a private company. She is at her second gesture (pregnancy) and mother of a year old boy.
She is admitted to maternity for childbirth since Saturday and we meet on Monday or 48 hours after admission. According to information received from the medical service, Bokoy is 38 weeks pregnant, so she is definitely over. Her partogram indicates a normal pregnancy with a fetus in good shape. Since its dilation is only two fingers since its admission and contractions intermittently in a very slow rhythm, they are called false contractions or lack of contractions. As a result, we started our psychological counseling protocol.
Psychodynamic interview: In seeking to discover the problem that has prevented the evolution of the Bokoy childbirth process for two days, despite the placement of the artificial induction of labor (theobald), we began by asking her to tell us the age of her first child. When Bokoy told us he was one year old, we went on to find out how she felt when she found out that she was pregnant when her baby was only 3 months old. “I felt very ashamed and worried. I wanted to find another solution,” she told us in a very anguished tone. “Another solution, which one?” We asked her. She will finally tell us that she wanted to abort twice by swallowing a high dose of quinine but without success. She finally decided to keep this pregnancy despite her until the end.
For us, this admission was more than enough to block or disrupt this delivery. This is how we went to the phase of prophylactic psychoeducation.
Psychoeducational prophylaxis: After having obtained Bokoy’s confession of the psychogenic situation (the fact of having wanted to abort) that we supposed to be the cause of the blocking of the process of his delivery, we asked him to accept this child as a reality without guilt.
Pedagogically, we explained to Bokoy that the anxiety, guilt, worries and other emotions that a woman may experience or all the actions she takes during her pregnancy have a great impact on her delivery. Also, should she know that a child is a blessing and maybe this child could save her family in the future. In addition, Bokoy should understand that she and her husband have a great responsibility in the birth of this child. And the fact that she is late in giving birth is not a good thing for her.
On a psychological level, Bokoy should accept this situation and rejoice in bringing his child into the world. Maybe it was not her wish, but the fact that she tried to abort without success is not a coincidence. She should be prepared to give this child maternal affection and love. So she should understand that the outcome of her situation depended on herself.
From a behavioral point of view, it is a question of attitude and cooperation that Bokoy should show during this whole process of delivery both for her baby and for the nursing staff.
Psychological support: To support her psychologically and in accordance with our protocol of help, we first did some sessions of deep breaths with Bokoy in order to internalize the whole process of prophylactic psychoeducation and to have her start the process of childbirth without anxiety or a lot of stress. Then we taught him the technique of haptonomy which consisted in asking at first pardon his baby for wanting to get rid of him. Then, to say nice words like “I am ready to receive you, my baby, and I am waiting for you without delay”. This technique puts Bokoy and his child in harmony and allows psychic triggering of child labor.
Results: It took us about half an hour for Bokoy to resume her contractions quickly and after exactly one hour and a half, she gave birth to her daughter at 13:10. However, it should be noted that since Bokoy’s daughter was an albino, he had come back to us to accompany him psychologically to avoid the discrimination of albinos in several sub-Saharan African countries, including the DRC, my country.
Nono case
Nono is a 32-year-old multipart. She is the mother of three children and is 40 weeks pregnant. She arrived at the maternity with a work already advanced, 7cm dilation, but for two hours this work is stationary. This situation worries the doctor who follows Nono, thus asks for our help. We began our intervention with psychodynamic maintenance.
Psychodynamic interview: During our interview with Nono, we noted that she had her first daughter with a married man who had left her custody of the child. Thirteen years later, this man returned to Nono to claim his daughter while Nono is currently married to another man with whom she has two children and was going to give birth to a third. At the same time, Nono and her husband are in a precarious financial situation.
The pressure that the first man, father of the eldest daughter of Nono had to recover this girl and the social situation of precariousness that crosses Nono in his home, seem to be according to our reading, the factors favoring this stagnation of the labor of Nono.
As a result, we carried out prophylactic psychoeducation and psychological support to decant this situation.
Prophylactic Psychoeducational: This step consisted in explaining Nono that having conflicts with her first spouse who currently has her own family, with all the consequences of being assaulted by the man’s wife, and the financial situation in which she was in her home were the two main problems of her life that affected the normal evolution of her labor.
Psychologically, these purely physical conflicts engendered intra-psychic conflict in Nono to such an extent that she could not concentrate on her delivery. Nono feels guilty of her infidelity and thinks internally that she may have problems with her current husband. This overloaded mental state of Nono inhibits her contractions.
Behaviorally, Nono should turn her attention to the present moment, her delivery leaving all other problems out because her life and that of her baby depend on it.
Psychological support: Our help to Nono consisted of an episode of relaxation with alternating breaths, followed by the haptonomy technique in which Nono should focus totally on her baby, imagining how he was going down to get out of him. speaking. We had also asked Nono to place beside her ear, her phone in which was recorded beautiful music that she should listen gracefully.
Result: At the end of two hours, Nono made a eutocic delivery of a boy. And her joy was so great that the wise women with whom we were in the delivery room called us a magician, because they could not understand that with the word only we could start the process of childbirth. had already planted.
Conclusion
This study proposed to contribute to the Millennium Development Goals and the Sustainable Development Goals for the improvement of maternal health.
We felt that existing methods and strategies could be enriched with newness by tapping into our traditional African cultures where speech was an important tool in problem solving. This same, word is also the therapeutic weapon for clinical psychologists and psychotherapists, consisting in creating an abreaction by catharsis and unraveling psychic blockages.
With the aid protocol inspired by Luba-Kasai therapeutic practices, we have succeeded in demonstrating that it is possible to associate psychological care with the number of birthing aids, whether medical (pharmacological) or natural, so that, in a synergy of actions, we manage to deliver the woman in difficult situation during her chilbirth and thus limit the risk of maternal death.
This study will have the merits of integrating our complicated childbirth assistance protocol into the psychotherapy arsenal already in place, in order to rightly improve maternal health in childbirth.
The analysis of the results obtained during this study has just demonstrated that the psychological intervention is an appreciable contribution in the accompaniment of the pregnant woman from conception to delivery.
Our study will give, we hope, a new dimension to the psychological care with a practical protocol, simple to implement.
We are also of the opinion that this study will open up new horizons for obstetrician gynecologists and maternal wise women to put into practice the helping relationship, this ability to get people in difficulty to mobilize their resources to better live their situation. We hope it goes in line with Bradely S. and peers [7], when they recommend: “Future research should explore their perceptions of the value and practice of interpersonal aspects of maternity care and the impact of disrespectful care on their sense of professionalism and personal ethics.”
References
- Rogers C (2015) The Helping Relationship and Psychotherapy, France. ESF edition.
- Pedinielli JL (2009) Introduction to clinical psychology, Armand Colin.
- Benony H, Chahraoui (2003) Clinical Interview, ed. Dunod.
- Bouvet C, Boudoukha AH (2014) 22 major notions of clinical psychology and psychopathology, ed. Dunod.
- Renou M (2005) Psychoeducation, a conception, a Montreal: Edi- tions Sciences et culture.
- Boon H (1876) The Sophrology, A Revolution in Psychology, Pedagogy and Medicine, RETZ-C.E.P.L.
- Bradley S, McCourt C, Rayment J, Pharmar D (2016) Disrespectful intrapar- tum care during facility-based delivery in sub-Saharan Africa: A qualitative systematic review and thematic synthesis of women’s perceptions and expe- Soc Sci Med 169: 157-170.
Citation:Mamba AM (2018) Complicated Childbirth Aid Protocol In- spired by Luba-Kasai Therapeutic Practice. J Perina Ped 2: 006.
Copyright: © 2018 Mamba AM. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.