*Corresponding Author:
Abdou Niasse,
Department of Surgery, Pikine Hospital, Dakar, Senegal
Tel: +221 778084873
Email: niasseabdou30@gmail.com
Abstract
Rhabdomyomas are benign tumors of the striated muscles. Localized mainly in the heart, extracardiac forms in adults are often seen in the neck and head. Rhabdomyomas of the abdominal wall are rare often posing the problem of differential diagnosis with malignant tumors. We report a case of rhabdomyoma of rectus abdominis muscle in a 32-year-old patient who progressed well after surgical excision.
Conclusion: Rhabdomyoma of abdominal wall is rare. Its surgical excision seems to be a good therapeutic approach with a low risk of recurrence.
Keywords
Abdominal wall tumors; Rectus abdominis muscle tumor; Rhabdomyoma
Background
Rhabdomyomas are rare mesenchymal tumors made up of striated muscle cells. These tumors exist in two forms: cardiac and extracardiac [1]. It is a more common pathology in children often associated with tuberous sclerosis of Bourneville disease with a predominantly cardiac location [2]. For adult, extracardiac forms are localized mainly to the neck and the head. Its abdominal location is even rarer, which can pose the problem of differential diagnosis with other often malignant tumors [3,4]. We report a case of a 32-year-old woman, who presented with rhabdomyoma of the rectus abdominis muscle, prompting total resection with simple consequences.
Observation
She was a 32-year-old female patient with no particular medical history. She presented intermittent chronic pain in left hypochondrium without digestive or urinary disorders. Physical examination found android obesity with a BMI of 37 kg/m2. Hemodynamic constants were normals and abdominal palpation revealed a homogeneous painless fixed firm parietal mass of approximately 5 cm below the left rib margin. Biologicals examens were normals. The injected abdominal CT revealed a tissue lesion of left rectus muscle of 69 mm x 25 mm x 35 mm well limited, homogeneously enhanced in favor of a benign tumor (desmoid tumor or Rhabdomyoma) (Figure 1). Surgical excision of the mass under general anesthesia was performed (Figures 2 and 3). Following were simples. Histological examination returned in favor of a rhabdomyoma without signs of malignancy. After 19 months of follow-up, no recurrence was reported.
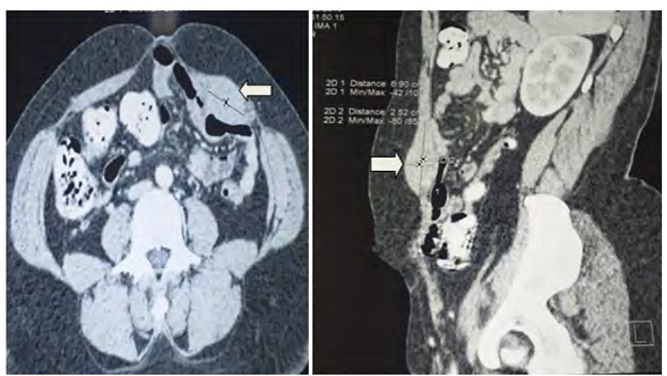
Figure 1: CT images of the tumor (white arrow) developed at the expense of the left rectus abdominis muscle of the abdomen.

Figure 2: Peroperative view tumor.
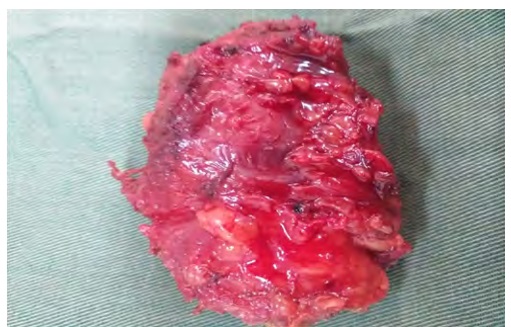
Figure 3: Operative piece.
Discussion
Adult-type rhabdomyoma is a rare benign tumor of skeletal striated muscle representing approximately 2% of striated muscle tumors [1,4]. These tumors are classified into cardiac and extracardiac forms. The extracardiac type is subdivided into three subtypes: vaginal, fetal and adult [5]. Often asymptomatic and slowly progressing, rhabdomyomas mainly affect men in their forties [6,7]. In women, vulvar location is the most frequent mimicking a fibroid or condyloma [3,8]. Adult-type rhabdomyomas are preferentially localized in the neck and head, in particular the soft palate, pharynx and submandibular region [1,4,9]. In children, cardiac localization is the most frequent often associated with tuberous sclerosis of Bourneville [10]. Its localization abdominal wall, as found in our patient, is very rare. Our patient was 32 years old. Steven and Oguntayo each reported a case of abdominal muscle wall rhabdomyoma in 37-year-old and 27-year-old patients, respectively, with no obvious etiology [1,3]. The rarity of these benign tumors often suggests primarily neoplastic lesions such as rhabdomyosarcomas. While a malignant tumor of abdominal musculature is often taken into account, injected computed tomography and magnetic resonance imaging have made it possible to clearly characterize the rhabdomyoma in the form of a respectively hyperdense and hyper intense muscle structure homogeneous with the absence of invasion of surrounding structures [4,5]. Histologically, adult-type rhabdomyoma is an encapsulated, polylobed and homogeneous macroscopic tumor. Buff colored, it is made up of well differentiated striated muscle cells with an eosinophilic abundant cytoplasm with numerous mitochondria and glycogen granules. There are focal areas of thick myofibrils rich in myosin and fine actin. It is the obvious striated muscle differentiation of tumor cells that characterizes the adult type. Mitoses are absent [9]. In our patient, the indication for surgical excision from the outset without a first biopsy was justified by the painful symptoms and the lack of consensus for possible monitoring or first biopsy. Majority of authors advocate that rhabdomyomas should only be treated if they become symptomatic and in the least aggressive way possible [1,3- 5]. Choice of technique and first voice depend on the tumor location [4]. Their complete excision is treatment of choice and helps prevent recurrence. Clinical and radiological monitoring of this type of lesion must be prolonged because late recurrences have been observed eight years after surgery. This risk of recurrence varies according to the authors between 16 and 42% in the event of incomplete surgery [9,10].
Conclusion
Extracardiac rhabdomyomas are unusual and can be mistaken for malignant muscle tumors. Their localization on abdominal wall is even rarer. However, imaging can characterize this benign lesion and also guide the initial and surgical excision which remains the cornerstone of the management of this pathology.
References
- 1. Steven A, Giuseffi Mark A, Gonzalo M (1983) Rhabdomyoma of the abdominal wall: Resection based upon computerized J Surg Oncol 22: 1-4.
- 2. Favia G, Lo Muzio L, Serpico R, Maiorano E (2003) Rhabdomyoma of the head and neck: Clinicopathologic features of two Head Neck 25: 700-704.
- 3. Oguntayo AO, Adesiyun AG, Onwuhafu PI (2006) Anterior abdom- inal wall rhabdomyoma mimicking fibroid: A case report. Nigeria Journal of Surgical Research 8: 3-6.
- 4. Bizon A, Capitain O, Girault S, H. Charrot, Laccourreye L (2008) Multifocal adult rhabdomyoma and positron emission tomography. Ann Otolaryngol Chir Cervicofac 125: 213-217.
- 5. Delides A, Petrides N, Banis K (2005) Multifocal adult rhabdomyo- ma of the head and neck: A case report and literature review. Eur Arch Otorhinolaryngol 262: 504-506.
- 6. Moriniere S, Sibel JP, Marlier, F, Guerrier B (2001) Basilingual rhab- domyoma treated by endoscopy. Ann Otolaryngol Chir Cervicofac 118: 245-248.
- 7. Liess BD, Zitsch AP, Lane R, Bickel JT (2005) Multifocal adult rhab- domyoma: A case report and literature Am J Otolaryngol 26: 214-217.
- 8. Iversen UM (1996) Two cases of benkgn vaginal rhabdomyoma. Case reports. APMIS 104: 575-578.
- 9. Kapadia SB, Meis JM, Frisman JM, Ellis GL, Heffner DK, et al. (1993) Adult rhabdomyoma of the head and neck: a clinicopatho- logic and immunophenotypic study. Hum Pathol 24: 608-617.
- 10. Samujh R, Dharmik A, Joshi K, Rao KLN (2004) Fetal rhabdomyo- ma in a neonate. Indian Pediatr 41: 839-842.
Citation:Niasse A, Faye PM, Ndong A, Gueye O, Sarr ISS, et al. (2021) Rhabdomyo- ma of Abdominal Wall: A case Report. J Case Repo Imag 5: 033.
Copyright: © 2021 Niasse A, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
