*Corresponding Author:
Baktash Morrad,
Department of Cardiology, Eskişehir Osmangazi University, Eskişehir, Turkey
Tel: +90 5074802729
E-mail: dr.bektash@hotmail.com
Abstract
Objective: Investigation of the incidence of arrhythmias and association of arrhythmia with gender in the early period in patients diagnosed with acute coronary syndrome and treated with percutaneous revascularization.
Subject and methods: Patients diagnosed with acutec oronary syndrome (unstable angina pectoris, non ST elevation myocardial in farction, and ST elevation myocardial in farction) were enrolled in the study prospectively. The rhythm analyses of the patients admitted in the coronary care unit were assessed by examining the 48 hour electro cardiography recordings via telemetry. The patients were divided into two groups regarding their genders as males, and females. The two groups were compared in terms of the incidence of development of arrhythmia.
Results: Seven hundredand ten patients with acute coronary syndrome enrolled in thestudy. Of these patients 155 (21.8%) were identified with supraventricular and ventricular arrhythmia. In final analyses, the average age of these identified patients (46 females, 109 males) were 65.6±12.8. The total incidence of development of arrythmia regarding the sub groups of acute coronary syndrome were likewise in males and females (p=0.57). Ventricular fibrillation was detected in 2.67% and permanent ventricular tachycardia in 5.7% of the patients. The frequency of permanent ventricular tachycardia andventricular fibrillation were likewise in males and females (p=0.64). The incidence of premature atrial beats in males were more of ten than in females, 18.3% and 6.5% respectively (p=0.03). The development of atrial fibrillation in females was seen more often than in males, 32.6% and 18.3% respectively (p=0.002).
Conclusion: The development of life threatening malignant ventricular arrhythmias (ventricular tachycardia and ventricular fibrillation) were the same in both genders. Early reperfusion therapy in patients diagnosed with acute coronary syndrome can reduce the incidence of all types of arrhythmias in both genders.
Keywords
Acute coronary syndrome; Arrhythmia; Gender
Introduction
Cardiovascular diseases are the leading cause of death worldwide [1]. Coronary artery disease and its subdivision, acute coronary syndromes, account for the most important causes of morbidity and mortality due to cardiovascular diseases [2]. Acute coronary syndromes are divided into three major groups: unstable angina pectoris, non ST segment elevation myocardial infarction, and ST segment elevation myocardial infarction [3]. The most important mechanism responsible for development of acute coronary syndrome is acute occlusion of coronary arteries with varying degrees as a result of adhesion and aggregation of material rich in thrombocyte and fibrin due to tearing and/or wearing off in atherosclerotic plaque [4].
The most important causes of death in patients with acute coronary syndrome are arrhythmogenic complications and development of cardiogenic shock. The most common causes of death during first few hours before reaching a hospital in patients with acute coronary syndrome are malignant arrhythmias such as ventricular tachycardia and ventricular fibrillation. In 50% of acute ST segment elevation myocardial infarctions, sudden death due to ventricular tachycardia and ventricular fibrillation is the first finding of the disease [5,6]. During hospitalization, however, degree of impairment of left ventricular functions is the most important factor related to death. There are limited number of studies in literature suggesting that presence of arrhythmia during hospitalization is related to an increase in mortality and morbidity in patients with acute coronary syndrome. Besides, there is not sufficient information in literature regarding the prevalence of arrhythmia development during the course of acute coronary syndrome. In scarce number of studies conducted on this topic, different results were reported (varying between 0.3% and 18%) about arrhythmia [7,8].
In this study, the aim was to investigate the prevalence of arrhythmia development during early period and relationship between arrhythmia development and gender in patients who were admitted with diagnosis of acute coronary syndrome and who underwent percutaneous revascularization intervention.
Material and Methods
This study was conducted prospectively, and 710 patients who admitted to coronary intensive care unit with the diagnosis of acute coronary syndrome between December 2012 and May 2014 were included in the study. Local ethical committee approval and informed consent from all patients were obtained for the study.
Patients with acute coronary syndromes (unstable angina pectoris, non ST segment elevation myocardial infarction, and ST segment elevation myocardial infarction) were included in the study. Exclusion criteria were as follows: patients with previous myocardial infarction, history of cerebrovascular event, previous coronary bypass surgery or percutaneous coronary intervention procedure, known atrial fibrillation/flutter, presence of pregnancy and development of acute coronary syndrome during peripartum period, patients with malignancy and those who did not undergo coronary angiography.
Rhythm analysis of patients with acute coronary syndrome who were admitted to coronary intensive unit was evaluated using telemetry records (Nihon-Kohden BSM 4113 K, Nihon-Kohden Corporation, Tokyo, Japan) and first 48 hours electrocardiography records. Presence and prevalence of arrhythmia from telemetry record were examined by a cardiologist experienced in arrhythmia and patients were unaware of this.
Identification of Arrhythmias
Tachyarrhythmias
Ventricular extra systoles: Premature beats with wide QRS complex (≥120 ms) occurring before the expected time were defined as ventricular extra systole; ventricular premature beats occurring less than 50 beats per hour were excluded from the study.
Ventricular tachycardia: Ventricular tachycardia was defined as ventricular premature beats occurring three or more times repeatedly with a heart rate faster than 100 beats/min and with wide QRS complex (≥120 msn). Ventricular tachycardias that do not lead to hemodynamic impairment or last less than 30 seconds were defined as nonsustained tachycardia, whereas tachycardias that last longer than 30 second or those lead to hemodynamic collapse regardless of their duration were defined as sustained tachycardia.
Polymorphic sustained ventricular tachycardia: was defined as Torsades de pointes [9].
Ventricular fibrillation: Entirely asynchronous ventricular rhythms with a rate of >300 beats/min that had highly variable QRS rate, morphology and amplitudes were defined as ventricular fibrillation.
Atrial extra systoles: Was defined as atypical QRS complex having short or long PR intervals, depending on site of origin, narrow QRS following normal QRS different than P wave. Patients who had atrial premature beats <50 beats/hour were excluded from the study.
Atrial flutter: Supraventricular tachycardias without P waves, having regular QRS intervals, in which Flutter (F) waves with an atrial rate of 240-340 beat/min were defined as atrial flutter.
Atrial fibrillation: Supraventricular rhythms with narrow and irregular QRS complexes and f waves with atrial rate of 350-600 beats/min and no p waves were defined as atrial fibrillation.
Brady arrhythmias
1st Degree atrioventricular block: was defined as normal QRS complex with a PR interval of >200 ms.
2nd Degree atrioventricular block: Second degree atrioventricular block was not divided according to its types; it was defined as P without QRS response without PR interval prolongation or following a gradual prolongation of PR interval.
3rd Degree atrioventricular block: Third degree atrioventricular block is an arrhythmia where P waves and QRS complex are regular in their own, and P waves have no relation with QRS waves and heart beat is <40-60 beat/min.
Asystole: Was defined as ventricular rhythm in which electrical activity is disappeared and there in not any P wave or QRS complex.
All primary percutaneous coronary intervention processes were conducted using conventional techniques. Stent/balloon option or preferences regarding complementary treatment interventions were left to operator’s choice. All of our patients in our study group were given anti-ischemic and antiaggregant treatment compatible with current guidelines. Beta blockers were initiated in all patients, except where contraindicated, and optimal standard dosages were tried to be attained.
Hematologic and biochemical studies were done in all participants at their first admittance. Increase and decline of values of creatine kinase-MB and troponin T that are among the markers for myocardial necrosis, was assessed over time. Once clinical stabilization was achieved, patients underwent transthoracic echocardiography and left ventricle functions were evaluated.
Patients were divided into two groups as females and males according to their gender. Comparisons were done among the groups in terms of prevalence of arrhythmia development.
Statistical analysis: Continuous variables were expressed as mean ± Standard Deviation (SD), while categorical variables were expressed as percentage. Student t test was used in comparison of continuous variables that display normal distribution, and Mann Whitney U test was used in comparison of non normally distributed variables. p<0.05 value was considered as significant in all comparisons. Statistical analyses were done using SPSS 16, 0 program (SPSS Inc., Chicago, IL).
Results
Supraventricular and ventricular arrhythmia, which were defined in methods section, were detected in 155 (21.8%) of 710 patients with acute coronary syndrome who were included in this study. Final analyses were done on these 155 patients with arrhythmia. The average age of 155 patients (46 female, 109 male) was 65, 6 ± 12.8. Female patients were older (74.1±11.5) than male patients (61.9±11.5) (p=0.001). Hypertension, family history and smoking, which are among the cardiovascular risk factors, were more common in male patients than female patients (p=0.002). Killip score was 1 in 79.4% of the patients with arrhythmia, it was 2 in 3.2%, 3 in 5.8% and 4 in 11.6%. When it was assessed according to sex status, Killip score was poorer in male patients compared to female patients (p=0.002). Basic clinical and demographic characteristics of study population were summarized in table 1.

Table 1: Basic clinical and demographic characteristics of study population.
DM: Diyabetis Mellitus, HT: Hipertansiyon, ACE: Angiotensin Converting Enzyme, RAS: Renin Angiotensin System, KKB: Kalsiyum Kanal Blokeri, ASA: Asetil Salisilik Asit.
Both supraventricular and ventricular arrhythmias occurred most often in patients with ST segment elevation myocardial infarction, followed by non ST segment elevation myocardial infarction and least commonly in patients with stable angina pectoris. Prevalence of arrhythmia development according to acute coronary syndrome subtypes was similar in females and males. Prevalence of arrhythmia according to acute coronary syndrome subtypes was shown in graph 1.
Graph 1: Prevalence of arrhythmia according to acute coronary syndrome subtypes.
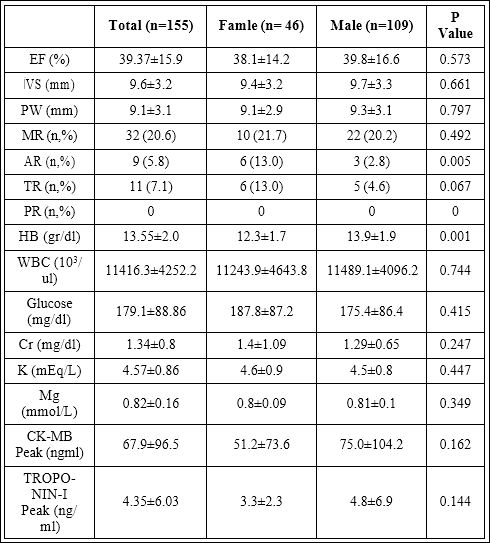
Once clinical stabilization was achieved (mean 1,8 days), patients underwent transthoracic echocardiography examination. Left ventricle systolic functions were similar in females and males. Aortic insufficiency was less common in male patients (2.8%) compared to female patients (13%). Hemoglobin values were lower in women (12.3±1.7 mg/dl) than in man (13.9±1.9 mg/dl) (p=0.001). Blood electrolytes and markers for necrosis, which show the size of the myocardial necrosis were not significantly different in both genders. Basic echocardiographic and hematologic results of study population were summarized in table 2.
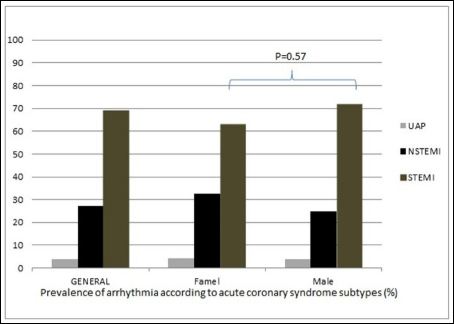
Table 2: Basic echocardiographic and hematologic of results of study population.
EF: Ejection Fraction, İVS: İnterventricularseptum, PW: Posterior Wall, MY: Mitral regurgitation, AR: Aorticredurgitation, TR: Tricuspitregurgitaiton, PR: Pulmonaryregurgitation, HB: Hemoglobin, WBC: White Bloodcell, Cr: Creatinin, K: Potassium, Mg: Magnesium, CK-MB: Creatinikinase MB.
Analysis was done for each arrhythmia type according to gender group. Frequent atrial premature beat development was more common in males (18.3%) than in females (6.5%) (p=0.03). Atrial fibrillation occurred less in males (18.3%) than in females (32.6%) (p=0.002). Other supraventricular and ventricular arrhythmias occurred in similar frequency in both genders. Results regarding prevalence of supraventricular and ventricular arrhythmias according to gender were summarized in table 3.
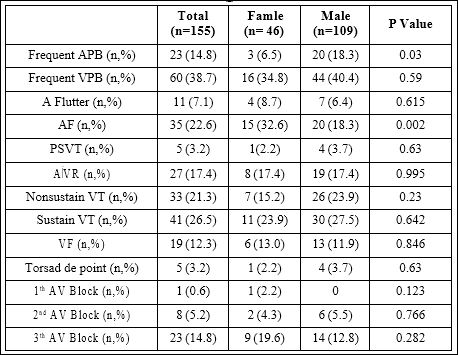
Table 3: Results regarding prevalence of supraventricular and ventricular arrhythmias according to gender.
APB: Atrialprematurebeat, VPB: Ventricular Primaturebeat, A flutter: Atrialflutter, AF: Atrial Fibrilation, PSVT: Paroksismal Supraventricular Tachicardia, AİVR: Akseleratedidiyo Ventricular Rhythm, VT: Ventricular Tachicardia, VF: Ventricular Fibrilation, AV: Atrio Ventricularblock.
Analysis was done for each arrhythmia type according to acute coronary syndrome type. Frequent ventricular early beat development was found in 46.7% of the patients with ST segment elevation myocardial infarction, while it was detected in 23.8% of patients with non ST segment elevation myocardial infarction (p=0.005). Atrial flutter was more common in non ST segment elevation myocardial infarction group (19%) compared to ST segment elevation myocardial infarction group (2.8%) (p=0.002). Accelerated idioventricular rhythm was more common in patients with ST segment elevation myocardial infarction (22.4%), as expected (p=0.002). There was not any difference among other groups in terms of acute coronary syndrome type. Results regarding prevalence of arrhythmia according to acute coronary syndrome type were summarized in table 4.
Discussion
In this study, prevalence of arrhythmia development and relationship between arrhythmia and gender factor was investigated in patients who were hospitalized in Coronary Intensive Care Unit (CICU) because of Acute Coronary Syndrome (ACS). Presence of arrhythmia was evident in 21% of the population studied. Arrhythmia was most common in ST Segment Elevation Myocardial Infarction (STEMI), followed by Non ST segment Elevation Myocardial Infarction (NSTEMI) and Unstable Angina Pectoris (UAP).
Almost all types of arrhythmias can be seen during course of acute coronary syndrome. Prevalence of arrhythmia during course of acute coronary syndrome was highest in STEMI, followed by NSTEMI and UAP. In our study, prevalence of arrhythmia depending on acute coronary syndrome was consistent with previous studies [10]. In patients with STEMI, almost all types of arrhythmia can develop during acute phase of the infarction. It was shown in several studies that arrhythmias develop most frequently during the first 24 hours of onset of the infarction [11-14].
Most common ventricular arrhythmias during course of acute coronary syndrome are Ventricular Premature Beats (VPB). If not complex in morphology, VPB is considered as clinically insignificant. However, studies conducted on ACS revealed interesting findings about VPB. In a study conducted by Winkler et al., >50/hour VPB was observed in 22% of the patients with ACS during 24 hours of miniaturization. This study showed that frequent VPB increased the recurrent hospitalizations [15]. In our study, >50/hour VPB was observed in 38.7% (8.4% of 710 patients) of patients with diagnosis of acute coronary syndrome. In 46.7% of the patients (6.6% of 710 patients) with STEMI, >50/hour VPB was observed. Prevalence of VPB in our study is consistent with the data in literature.
Leading causes of death during early phase of acute coronary syndrome are malignant ventricular arrhythmias such as Ventricular Tachycardia (VT) and ventricular fibrillation [5,6]. In Global Registry of Acute Coronary Events study, one of the biggest studies done on this subject, ventricular arrhythmia was detected in 6.9% of the >50,00 patients presented with ACS (1.8% VT and 5.1% VF). When analyzed according to acute coronary syndrome type, ventricular arrhythmia was seen in 12% of STEMI, in 4.9% of NSTEMI and in 3.1% of UAP. Ventricular arrhythmias developed within the first hour in 80% of these patients. Same study reported that mortality was significantly higher in patients who developed arrhythmia during hospitalization or on six months following discharge [16]. Another study suggested that VT was present in 6%, and VF was present 4 to 20% of the patients. In this study, ventricular arrhythmias prolonged hospital stay time significantly [15]. In our study VF was found in 2.67% of the 710 patients who were admitted to CICU with acute coronary syndrome diagnosis; sustained VT was detected in 4.36% of the patients and nonsustained VT was found in 4.36% of the cases. Prevalence of VT and VF is a little less than other studies conducted on this topic. We believe that this might have some reasons. As mentioned in methods part, percutaneous revascularization of the vessel responsible for acute ischemia was carried out in all patients who were admitted to CICU in our study. It is well known that myocardial ischemia is the most important reason for development of ventricular arrhythmia. As a consequence, we believe that disappearance of ischemic condition might have an impact on lower prevalence of VT/VF. Development of arrhythmia during course of ACS is also affected by medical treatment beside reperfusion treatment [17]. Beta blocker treatment started early during the course of ACS decreases prevalence of arrhythmia. In our study population, beta blocker treatment was started in all patients unless there was a contraindication, and optimal dosage was achieved as much as patients could tolerate. We also think that anti ischemic treatment has an impact on prevalence of arrhythmia development.
Most common supraventricular arrhythmias during course of acute coronary syndrome are Atrial Premature Beats (APB). It is now well known that frequent presence of APB is a risk factor for Atrial Fibrillation (AF). Prevalence of APB was found to be higher in patients with coronary disease compared to those who do not have it. Frequent occurrence of APB during course of acute coronary syndrome is not an innocent condition. It poses a risk for future cardiovascular event and for development of AF [18]. Frequent APB was detected in 3.23% of the patients. There was not any difference in prevalence of APB in terms of acute coronary syndrome subtype and gender. Prevalence of APB in our study was similar to previous studies [17].
Atrial fibrillation is a disease that affects lifespan and quality of life. Its prevalence gradually increases with age. ACS is a strong risk factor that leads to atrial fibrillation due to ischemia. AF is seen in every 5 patients hospitalized with the diagnosis of ACS [18,19]. Barring atrial and ventricular premature beats, AF is the most common arrhythmia type that arises during ACS. Particularly STEMI subtype of ACS is associated with AF in 6.54 to 7.9% of the cases. This rate can reach up to 21%, if left ventricle systolic dysfunction is developed during course of myocardial infarction [20]. In The cardiac arrhythmias and risk stratification after acute myocardial infarction study, one of the largest studies on this topic, showed that new atrial fibrillation develops in 6% to 28% of the cases [21,22]. In our study, AF was detected in 4.92% of the patients. There was not any significant difference in AF prevalence in terms of acute coronary syndrome subtype, while when gender was taken into account, females had a higher rate of AF development (18.3% vs 32.6%, p=0.003). The study titled gruppo italiano per lo Studio della sopravvivenza nell. Infar to miocardico 3 also reported that AF was more common in women. We believe that high prevalence of AF in women can be associated with older age of women patients compared to men. Since development of ACS is expected to be later compared to men, no statistical adjustment was made in evaluation of the results.
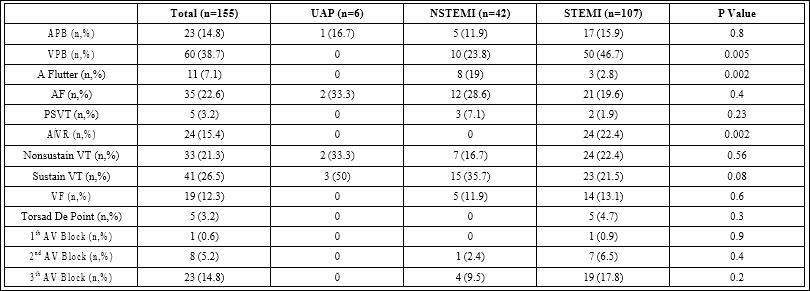
Table 4: Results regarding prevalence of arrhythmia according to acute coronary syndrome type.
APB: Atrial Premature Beat, VPB:Ventricular Primature Beat, A flutter: Atrial flutter, AF: Atrial Fibrilation, PSVT: Paroxysmal Supraventricular Tachycardia, AİVR: Akselerasi Ventricular Rhythm, VT: Ventricular Tachicardia, VF: Ventricular Fibrilation, AV: Atrio Ventricularblock.
Atrioventricular (AV) blocks of all degrees are seen more common in inferior myocardial infarction subtype of acute coronary syndrome. Most important reason for this is exposure of sinoatrial node and AV node to ischemic condition. In our study, AV block (1st, 2nd and 3rd degree AV block) prevalence was found as 0.14% 1.12% and 3.2%, respectively. These rates are lower than those reported in literature [23]. We believe that reason for lower prevalence of AV block in our study could be due to recovery of ischemia thanks to early reperfusion treatment.
When evaluating the results of our study, some of limitations of the trial should be considered. Since our study was conducted in one center, results cannot be generalized for the whole country, multicenter studies on this topic are needed. Patients admitted to our center could consist of those with high risk because the institution that our study was conducted was a tertiary center, however we do not have any evidence to support this hypothesis. Number of patients with acute coronary syndrome who were investigated for prevalence of arrhythmia might be insufficient. Further studies with higher number of patients could be more guiding.
As a consequence, development of lethal Ventricular Arrhythmia (VT/VF) that threatens life was found to be similar and low in prevalence in both genders. Early reperfusion treatment in female and male patients who were admitted for acute coronary syndrome can decrease occurrence of all arrhythmia types.
References
- Murray CJ, Lopez AD (1997) Alternative projections of mortality and disability by cause 1990-2020: Global Burden of Disease Study. Lancet 349:1498-1504.
- Hamm CW, Bassand JP, Agewall S, Bax J, Boersma E, et al. (2011) ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: The Task Force for the management of acute coronary syndromes (ACS) in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J 32: 2999-3054.
- Thygesen K, Alpert JS, Jaffe AS, Simoons ML, Chaitman BR, et (2012) Third universal definition of myocardial infarction. Eur Heart J 33: 2551-2567.
- Bassand JP, Hamm CW, Ardissino D, Boersma E, BudajA, et al. (2007) Guidelines for the diagnosis and treatment of non-ST-segment elevation acute coronary syndromes. Eur Heart J 28: 1598-1660.
- Wellens HJJ, Brugada P (1987) Cardiac Arrhythmias: Where to Go from Here? Futura Publishing Company, Austin, TX, USA.
- Zerkowski H-R, Baumann G (2006) HerzAkutMedizin: Ein Manual für die kardiologische, herzchirurgische, anästhesiologische und internistische Praxis, Springer Verlag, Berlin, Germany.
- Rosenfeld LE (1988) Bradyarrhythmias, abnormalities of conduction, and indications for pacing in acute myocardial Cardiol Clin 6: 49-61.
- Gorenek B, Lundqvist CB, Terradellas JB, Camm AJ, Hindricks G, et al. (2015) Cardiac arrhythmias in acute coronary syndromes: position paper from the joint EHRA, ACCA, and EAPCI task force. EuroIntervention 10: 1095-1108.
- Choudhuri I, Pinninti M, Marwali MR, Sra J, Akhtar M (2013) Polymorphic ventricular tachycardia-part I: structural heart disease and acquired causes. Curr Probl Cardiol 38: 463-496.
- Furman MI, Dauerman HL, Goldberg RJ, Yarzebski J, Lessard D, et al. (2001) Twenty-two year (1975 to 1997) trends in the incidence, in-hospital and long-term case fatality rates from initial Q-wave and non-Q-wave myocardial infarction: a multi-hospital, community-wide perspective. J Am Coll Cardiol 37: 1571-1580.
- Braunwald E (1997) Heart disease: a textbook of cardiovascular medicine. (5thedn), Saunders, Philadelphia, USA.
- Mangrum JM (2001) Tachyarrhythmias associated with acute myocardial in Emerg Med Clin North Am 19: 385-395.
- Al-Khatib SM, Granger CB, Huang Y, Lee KL, Califf RM, et al. (2002) Sustained ventricular arrhythmias among patients with acute coronary syndromes with no ST-segment elevation: incidence, predictors, and Circulation 106: 309-312.
- Guidry UC, Evans JC, Larson MG, Wilson PW, Murabito JM, et al. (1999) Temporal trends in event rates after Q-wave myocardial infarction: the Framingham Heart Circulation 100: 2054-2059.
- Adgey AA, Allen JD, Geddes JS, James RG, Webb SW, et al. (1971) Acute phase of myocardial infarction. Lancet 2: 501-504.
- Avezum A, Piegas LS, Goldberg RJ, Brieger D, Stiles MK, et (2008) Magnitude and prognosis associated with ventricular arrhythmias in patients hospitalized with acute coronary syndromes (from the GRACE Registry). Am J Cardiol 102: 1577-1582.
- Görenek B, Kudaiberdieva G, Lip G (2015) What we have learned from the ESC position paper on arrhythmias in acute coronary syndromes. Anatol J Cardiol 15: 94-96.
- Bigger JT Jr, Fleiss JL, Kleiger R, Miller JP, Rolnitzky LM (1984) The relationships among ventricular arrhythmias, left ventricular dysfunction, and mortality in the 2 years after myocardial Circulauon 69: 250-258.
- Saczynski JS, McManus D, Zhou Z, Spencer F, Yarzebski J, et al. (2009) Trends in atrial fibrillation complicating acute myocardial infarction. Am J Cardiol 104: 169-174.
- Kudaiberdieva G, Gorenek B (2007) Post PCI atrial fibrillation. Acute Card Care 9: 69-76.
- Bloch Thomsen PE, Jons C, Raatikainen MJ, Moerch Joergensen R, Hartikainen J, et al. (2010) Long-term recording of cardiac arrhythmias with an implantable cardiac monitor in patients with reduced ejection fraction after acute myocardial infarction: the Cardiac Arrhythmias and Risk Stratification After Acute Myocardial Infarction (CARISMA) study. Circulation 122: 1258-1264.
- Winkler C, Funk M, Schindler DM, Hemsey JZ, Lampert R, et al. (2013) Arrhythmias in patients with acute coronary syndrome in the first 24 hours of Heart Lung 42: 422-427.
- Shirafkan A, Mehrad M, Gholamrezanezhad A, Shirafkan A (2009) Conduction disturbances in acute myocardial infarction: a clinical study and brief review of the Hellenic J Cardiol 50: 179-184.
Citation: Morrad B, Eraslan S, Gorenek B (2017) Prevalence and Types of Supraventricular and Ventricular Arrhythmias Developing in Patients with Acute Coronary Syndrome. J Cardio Cardiovasu Med 2: 004.
Copyright: © 2017 Morrad B, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
