*Corresponding Author:
Doniparthi Pradeep,
Department of Cardiothoracic and Vascular Surgery, All India Institute of Medical Sciences, New Delhi, India
Tel: +91 9501626593
E-mail: pradeepdhoni023.pd@gmail.com
Abstract
With advancements in extracorporeal technology growing in leaps and bounds, intracardiac repair for complex congenital lesions are becoming easier day by day. Despite these advancements, pulmonary artery banding owes its own domain where at times, definitive repair is not possible. One should have a thorough knowledge of the physiology of the pulmonary artery band to avoid detrimental effects on circulationt.
Keywords
Circulation; Extracorporeal technology; Pulmonary artery band
Introduction
The author was asked by the junior co-trainee regarding the purpose of open chest instruments set beside a patient of an immediate post operative Pulmonary Artery Band (PAB) patient in the ICU (Intensive care unit) although it is a closed heart procedure.
Despite the technical ease of performing closed heart procedures in congenital cardiac surgery when compared to other open-heart procedures, the PAB definitely commands a higher place in the learning curve. One has to understand the quantum of PAB surgery as it was placed in category 3 of RACHS (Risk Adjustment for Congenital Heart Surgery) score, whereas open-heart procedures like Atrial Septal Defects (ASD) and Ventricular Septal Defects (VSD) and Tetralogy of Fallot (TOF) Repairs are placed in categories 1 and 2 [1].
Since the palliation of cyanotic children using Blalock Taussig Shunt in 1944, a huge milestone in the timeline of Congenital Cardiac Surgery is attributed to Muller, a Johns Hopkins Trainee, who in 1951, from the University of Virginia first described PAB.
Now a days the indications of PAB are decreasing due to increased understanding of the Cardiopulmonary Bypass (CPB) that has led to early definitive correction of congenital heart lesions, but certainly it is considered to be one of the landmark surgeries which palliated countless children before the era of open heart surgery with CPB [2-4]. The observations of the autopsy findings by Civin in an adult patient of TOF with a large VSD with infundibular stenosis whose pulmonary vascularity was protected from increased blood flow, thundered the idea of creating artificial pulmonary stenosis in the congenital lesions of increased pulmonary blood flow [5]. Muller and Duman’s procedure was similar to the original PAB, which consisted of a lateral tangential excision of the pulmonary artery along with wrapping of the artery with umbilical tape.
Although the technique worked well to palliate the patients, it was very difficult to balance the blood flow by tightening the band as the flow in a vessel is directly related to the fourth power of the radius according to the Poiseuille’s Law (Q=∏Pr4/8ηl). Reviewing the original experiments of Mann in 1939 on the relationship of the blood vessel’s diameter and flow, a reduction in flow of 50% was seen when the diameter of a vessel was reduced to 67%. This finding laid the foundation for the intricate balancing of the pulmonary (Qp) and systemic (Qs) circulations used in Banding Procedures [2]. The pulmonary artery band limits the blood flow to the pulmonary circuit hence Pulmonary Artery Pressure (PAP) is not the only surrogate marker to determine the adequacy of the band since flow is dependent on so many other factors like oxygen concentration, force of contraction of the ventricle, acid base status, effect of anaesthesia and many other things.
The concept of adjustable PAB by Noel in 1971 has attempted to solve the problem of band tightness to some extent but there was no definitive study to address this issue [6].
In order to maintain the balance between tight and loose bands, another momentous study was done by Trusler, who derived a formula to determine the tightness of the band by plotting a graph with the weight of the child and relief from failure symptoms in two sets of children, one with isolated VSD and another in Transposition of Great Arteries (TGA) with large VSD, in other words now familiar with biventricular physiology anduniventricular physiology respectively.
According to Trusler, the weight of the child (in Kgs) + 20 mm is adequate for the VSD group and the weight of the child (in Kgs) + 24 mm for TGA with VSD group was proposed. The extra edge of this 4mm is necessary for mixing in the TGA group. Although Trusler’s formula was not an accurate estimate in determining blood flow, it certainly helped to understand and estimate the tightness of the band [7]. Eventually, hemodynamic studies by Utley et al. In 1973, were eye openers for cardiac surgeons in terms of understanding the physiology of the PAB [8]. The purpose of pulmonary artery banding in biventricular physiology is to limit the excessive blood flow to the lungs (Qp) so that the work of breathing could be reduced and failure symptoms averted. Whereas in univentricular physiology the purpose of the PAB is to prepare the child for future Fontan pathway by protecting the lungs from developing irreversible pulmonary vascular changes (Table 1).
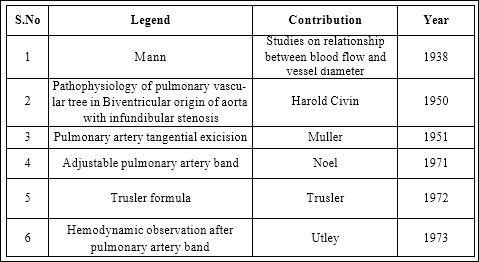
Table 1: Pulmonary vascular changes.
It is a delicate balance for the surgeon, who has to carefully tread this fine line, this two edged sword between the circulations of sys- temic and pulmonary vascular beds at the cost of right ventricular fail- ure (Tight band) and excessive pulmonary blood flow (loose band); particularly in univentricular physiology (Table 2).
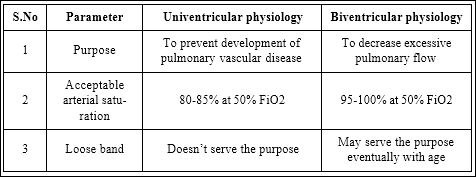
Table 2: Difference between Univentricular physiology and Biventricular physiology.
This is the author’s humble attempt to simplify the understanding of the pathophysiology of the PAB by comparing it with an electric circuit and near estimate of the tightness of the pulmonary artery band in univentricular physiology (figures 1 and 2).
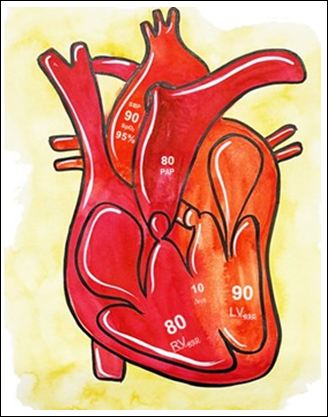
Figure 1A : In the scenario of Univentricular Physiology, a large, unrestrictive VSD causes the Right Ventricle (RV) to assume near normal systemic pressures ( Pressure Drop across the Ventricular Septum is 10).
These Systemic Pressures (SBP) are transmitted to the Pulmonary Arterial Tree and the goal of the Band (PAB) is to restrict such pressures so as to prevent the development of Pulmonary Artery Hypertension (PAH).
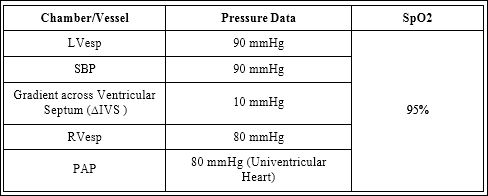
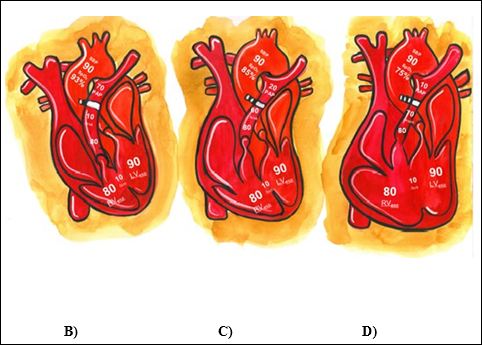
Figure 1B: In a Loosely Banded PA (band is tightened by 1 clip), the band offers min- imal resistance to the blood flow, which ultimately defeats the purpose in preventing the development of PAH.
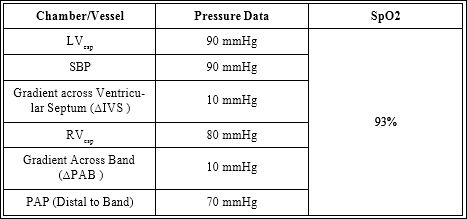
Figure 1C: In an adequately banded PA (band is tightened by 2 clips), the resistance offered by the band is adequate in preventing the development of PAH.
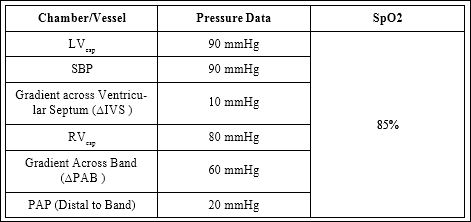
Figure 1D: In a tightly banded PA (band is tightened by 3 clips), the resistance offered by the band is too high, eventually resulting in (bulging of the RV) failure of the right ventricle.
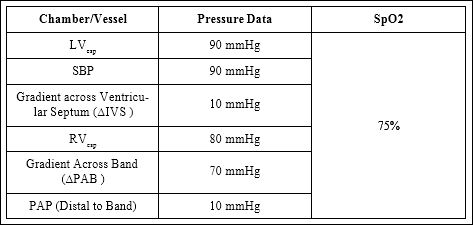
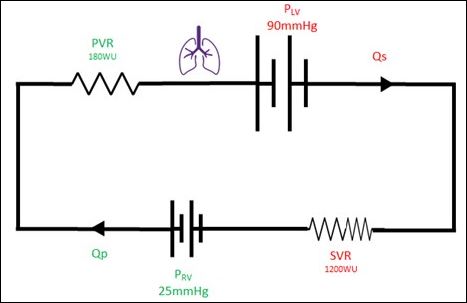
Figure 2A: Normal circulation.
Both systemic and pulmonary circulations are in series configuration with the same blood flow (Q). Hence PRV/PVR=PLV/SVR
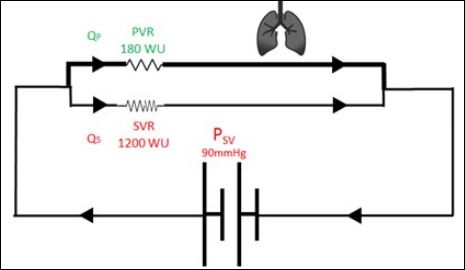
Figure 2B: Single ventricle physiology.
Both systemic and pulmonary circulations are in parallel configurationunder the same pressure head generated by single ventricle (PSV) and Qα 1/VR. Hence QP* PVR=QS*SVR or
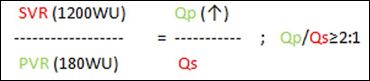
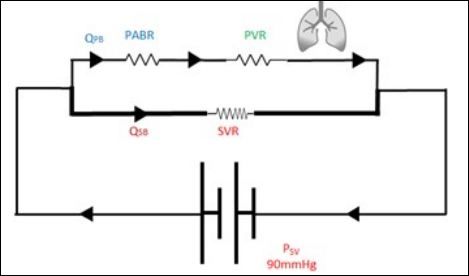
Figure 2C: Single ventricle physiology with banded pulmonary artery.
Both systemic and pulmonary circulations are in parallel configuration with the same pressure head generated by a single ventricle with extra resistance offered by PAB. Hence QP *(PVR+PABR) =QS*SVR or

Indications of pulmonary artery band [9]:
- Ventricular Septal Defect of the Swiss Cheese
- Univentricular Physiology with unrestricted Pulmonary Blood
- Delaying the decision between univentricular and biventricular repair in atrioventricular or ventricular septal defects with ventricular imbalance. Considering the Cohen’s ratio [10], an Atrio Ventricular Valve Index (AVVI) of <0.67, with Ductal Dependent Circulation and Non Ductal Dependent Circulation with AVVI between 0.27 to 0.67 with a large VSD should undergo Univentricular
- Increased pulmonary flow conditions with contraindications to cardiopulmonary bypass
- To restrict the pulmonary blood flow, to allow the child grow bigger(Bigger structures) for better biventricular physiology in conditions with complex lesions like common atrioventricular connection or a criss-cross heart.
- For preparing the left ventricle for future arterial switch operation in the late presenters of transposition of great vessels with an intact ventricular septum.
- Left ventricular preparation and/or reduction of tricuspid regurgitation in congenitally corrected transposition of great arteries with tricuspid regurgitation without sizeable VSD
- As an auxiliary procedure, (i) In bidirectional Glenn procedure, to limit the anterograde flow thereby reducing the pulsatility of flow.
- (ii) As a part of the palliative switch procedure in Tricuspid atresia with transposition of great vessels
Debatable indications:
- As a proposed strategy to preserve the left ventricular function for double switch procedure in congenitally Corrected Transposition of Great Arteries (ccTGA).
- As an adjuvant procedure along with physiological correction in the patient of ccTGA, for future anatomical correction.
- For reversing the pulmonary vasculopathy in patients with un- corrected congenital heart diseases with Eisenmenger syndrome (figure 3).
Conclusion
Pulmonary artery band is surgery with simplicity when compared to other intracardiac procedures, certainly it is a procedure with a complex pathophysiology deserving its own citadel. While intricacy in balancing the band can mean the difference between life and death in young patients, we must respect the physiology of the patient while confronting such scenarios.
References
- Simsic JM, Cuadrado A, Kirshbom PM, Kanter KR (2006) Risk adjustment for congenital heart surgery (RACHS): Is it useful in a single-center series of newborns as a predictor of outcome in a high-risk population? Congenit Heart Dis 1: 148-151.
- Nolan SP (1987) The origins of pulmonary artery bandings. Ann Thorac- Surg 44: 427-429.
- Kron IL, Nolan SP, Flanagan TL, Gutgesell HP, Muller WH Jr. (1989) Pulmonary artery banding revisited. Ann Surg 209: 642-647.
- Muller WH, Dammann J F (1956) Results following the creation of pulmonary artery Ann Surg 143: 816-821.
- Civin WH, Edeards JE (1950) Pathology of the pulmonary vascular I. A comparison of the intrapulmonary arteries in the Eisenmenger complex and in stenosis of ostiuminfundibuli associated with biventricular origin of the aorta. Circulation 2: 545-252.
- Fishman NH, Roe BB (1971) An adjustable pulmonary artery band. Arch Surg 102: 143.
- Trusler GA, Mustard WT (1972) A method of banding the pulmonary artery for large isolated ventricular septal defect with and without transposition of the great arteries. Ann Thorac Surg 13: 351-355.
- Utley JR (1973) Hemodynamic observations during and after pulmonary artery Ann Thorac Surg 15: 493-509.
- Sharma R (2012) Pulmonary artery banding: Rationale and possible indications in the current era. Ann Pediatr Cardiol 5: 40-43.
- Cohen MS, Jacobs ML, Weinberg PM, Rychik J (1996) Morphometric analysis of unbalanced common atrioventricular canal using two-dimensional J Am Coll Cardiol 28: 1017-1023.
Citation: Pradeep D, Malakar J, Saini GK (2022) How tight is Too Tight? Funambu- lism in Banding the Pulmonary Artery in Univentricular Hearts. J Cardio Cardiovasc Med 6: 029.
Copyright: © 2022 Pradeep D, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
