*Corresponding Author:
Kristopher Pfirman,
Department of Cardiology, The Medical Center at Bowling Green, Kentucky, USA
E-mail: kpfirman19@gmail.com
Abstract
Coronary arteries arising from a single ostium are a rare anatomical variant. If an interarterial course is present this may manifest as angina and even sudden cardiac death. In our case, the left main coronary artery arises from a single ostium in the right sinus of Valsalva those courses in an inferior and posterior fashion. The anomalous left main coronary artery runs posterior to the aorta and courses along the left atrium. High risk features were absent. Due to the benign nature of the lesion, the patient was treated medically for coronary artery disease.
Introduction
In the general population, the blood supply to the heart is supplied by the right coronary artery and the left main coronary artery which arise from two separate coronary cusps. However, congenital variations to this anatomy can occur. In this case we present a patient with such coronary artery anomaly.
History of Presentation
A male in his fifties with obesity, obstructive sleep apnea compliant with continuous positive airway pressure at night, hypertension, uncontrolled diabetes, ongoing tobacco use, dyslipidemia and a history of cerebral vascular accident presented with chest tightness, epigastric pain, shortness of breath with exertion, and increased palpitations. Previous echocardiogram revealed a left ventricular ejection fraction of >55%. A 7-day Life watch monitor revealed sinus rhythm with no documented arrhythmias. Given the recent normal nuclear stress test performed at an outside facility and atypical yet ongoing symptoms, the patient underwent a diagnostic left heart catheterization.
Cardiac catheterization was done given the patient’s high risk for Coronary Artery Disease (CAD) and chest pain complaints. The differential diagnosis would include occlusive coronary artery disease, Prinzmetal angina, microvascular coronary artery disease, coronary syndrome X, spontaneous coronary artery dissection, anomalous coronary artery with interarterial course. The coronary angiogram revealed an anatomic anomaly of the left main coronary artery (Figure 1). There was no obstructive CAD found. Coronary Computed Tomography Angiography (CTA) was subsequently ordered to further assess the anatomy and origin of the coronary arteries. CTA revealed a single coronary ostium with common origin of the right and left coronary arteries arising from the right sinus of Valsalva. The left coronary artery coursing posteriorly between the aortic root and left atrium, without an abrupt acute angle, intramural course, or fish-mouth ovoid appearance of the ostium (Figure 2).

Figure 1: Coronary Angiography: LAO 30 degrees. Single coronary ostium arising from the right coronary cusp. Anomalous left main coronary artery arising from the right coronary artery.
Due to the mild atherosclerotic presence identified on coronary angiography, the course of action was to manage medically using beta blockade and calcium channel blockade in addition to aspirin and statin therapy. Given the inferior and posterior course of the anomalous left main coronary artery, conservative management was elected. Given the lack of the intra-arterial course that would prove a risk to the patient, surgery such as coronary reimplantation or coronary unroofing was deferred. The patient was then to be followed up in the outpatient clinic two weeks post discharge.
Discussion
Association with current guidelines/position papers/current practice: The left main coronary artery was found to have an anomalous origin in the right coronary cusp. Clinical presentation of patients with coronary artery abnormalities range from asymptomatic to symptoms consistent with angina pectoris with possible sudden cardiac death, which is more common in young athletes [1]. It is estimated that up to 1.3% of the general population may have anomalous coronary artery origins [2]. Of this population, only 1.7% is estimated to have a single coronary artery arising from a solitary ostium (incidence of 0.0240.066%) [2]. It has been shown in postmortem studies that patients with the anomalous left coronary artery arising from the right sinus, around 59% will die before age 20, and death usually occurs with vigorous exertion [3]. Whereas the incidence of sudden cardiac death related to any coronary artery anomaly in the general population under 40 years old is 0.6% [3]. Anatomical factors in this case, such as the left coronary artery not taking an interarterial or intramural course, absence of an acute angle, or fish-mouth ostium, makes this a more benign variant.
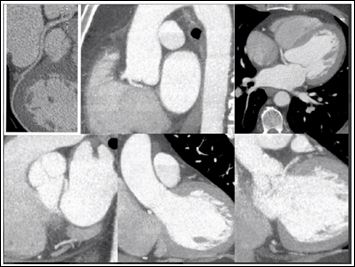
Figure 2: Coronary CTA images in the coronal, transverse, and sagittal planes revealing anomalous left main coronary artery from the right cusp of the sinus of Valsalva sharing a common ostium with the right coronary artery. The left main coronary artery takes aposterior and inferior course between the left atrium and aortic root.
Treatment for these anomalies is dependent on the course of the anomalous vessel [4,5]. That’s why classification of the anomaly is of the utmost importance, Lipton et al created the current classification system of single coronary arteries [2]. Coronary angiography is essential to establish the specific diagnosis [6]. Single coronary anomalies are usually asymptomatic, but an anomalous vessel which courses between the aorta and pulmonary trunk in an interarterial fashion is at high risk of compression, leading to anginal symptoms and possible sudden cardiac death [6,7]. These patients should receive referral to cardiothoracic surgery in order to bypass the vessel, reimplant the left coronary artery if able, or surgical unroofing of the vessel [8]. According to the 2018 AHA/ACC Guideline for the management of Adults with Congenital Heart Disease, surgery is a class one recommendation for symptoms or diagnostic evidence consistent with coronary ischemia attributable to the anomalous course of the coronary artery [9] There is a class IIa recommendation for anomalous origin of the left coronary artery from the right sinus in the absence of symptoms or ischemia or in the setting of ventricular arrhythmias [9].
Patients who have anomalous vessels which course around the great vessels and are not proceeding in an interarterial course are not at risk for compression and are therefore treated with conservative medical management as mentioned above. It should be noted that professional associations have issued guidelines that state untreated carriers of anomalous origins of a coronary artery should not be involved in strenuous activities at risk for sudden cardiac death that exhibit a dangerous course [8]. Once treated, a re-evaluation should be conducted before exercise is resumed [8]. Coronary artery anomalies should also be accurately documented to reduce potential harm when patients receive care from other providers, such as undergoing aortic valve replacement [1,8].
Given the course of the left main coronary artery not running in interarterial fashion, the patient was elected to be treated medically for non-occlusive coronary artery disease. The patient was followed in the outpatient setting without any recurrence of his original presenting symptoms.
Conclusion
Anomalous coronary arteries are a rare finding which can be discovered on cardiac catheterization. Management is based upon symptomology as well as anatomical course. Our patient was found to have a variant that was not clinically significant for sudden cardiac death and therefore was managed with conservative medical management.
Conflict of Interest
No conflicts of interest to be presented.
References
- Yamanaka O, Hobbs RE (1990) Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn 21: 28-40.
- Lipton MJ, Barry WH, Obrez I, Silverman JF, Wexler L (1979) Isolated single coronary artery: Diagnosis, angiographic classification, and clinical Radiology 130: 39-47.
- Angelini P, Velasco JA, Flamm S (2002) Coronary anomalies incidence, pathophysiology, and clinical Circulation 105: 2449-2454.
- Ozyurtlu F, Acet H, Bilik MZ, Tasal A (2012) A rare coronary artery anomaly: Single coronary artery originate from right sinus valsalva R-IIP subgroup Cardiology Research 3: 140-142.
- Ghersin E, Litmanovich D, Ofer A, Lessick J, Dragu R, et al. (2004) Anomalous origin of right coronary artery: Diagnosis and dynamic evaluation with multidetector computed tomography. J Comput Assist Tomogr 28: 293-294.
- Mustafa I, Gula G, Radley-Smith R, Durrer S, Yacoub M (1981) Anomalous origin of the left coronary artery from the anterior aortic sinus: A potential cause of sudden Anatomic characterization and surgical treatment. J Thorac Cardiovasc Surg 82: 297-300.
- Zingarelli A, Seitun S, Boccalini S, Balbi M. Bezante GP, et al. (2015) Anomalous single coronary artery (R-type) in the elderly: Description of benign and isolated Int J Cardiol 182: 10-12.
- Angelini P (2007) Coronary artery anomalies: An entity in search of an Circulation 115: 1296-1305
- Stout KK, Daniels CJ, Aboulhosn JA, Bozkurt B, Broberg CS, et (2019) 2018 AHA/ACC Guideline for the management of adults with congenital heart disease: Executive summary: A report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. Circulation 139: 637-697.
Citation: Pfirman K, Pham R, Haddad D, Donley C, Kazimuddin M, et al. (2020) Coronary Artery System Arising from a Solitary Coronary Ostium from the Right Sinus of Valsalva. J Cardio Cardiovasc Med 4: 019.
Copyright: © 2020 Pfirman K, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
