*Corresponding Author:
Amandeep Goyal,
Department of Internal Medicine, Marietta Memorial Hospital, Ohio, USA
Tel: +1 7404348258
E-mail: docaman2k1@live.com
Abstract
Aneurysm of the proximal left anterior descending artery has previously not been reported in D-transposition of the great arteries following an arterial switch operation. Arterial switch operation was performed on a male at 1 week of life that had D-transposition of the great arteries. Later in life, the patient was diagnosed with a proximal aneurysm of the left anterior descending artery. Patient also had an anomalous left circumflex artery originating from the right coronary artery, as well as an intramural course of the left anterior descending artery. This case highlights the management challenges posed by patients with congenital heart disease to general cardiology. A multidisciplinary management approach with proper transition of care is the best strategy for these patients.
Keywords
Congenital heart disease; Coronary aneurism; TGA; Transposition
Introduction
D-Transposition of the Great Arteries (D-TGA) is a congenital condition in which there is an abnormal conotruncal rotation during embryogenesis, resulting in ventriculo arterial discordance. This abnormal rotation results in the aorta arising from the right ventricle and the pulmonary trunk arising from the left ventricle, forming a parallel circulation not compatible with life without surgery. D-TGA is usually diagnosed prenatally or in the early postnatal period when neonates develop cyanosis. Arterial Switch Procedure (ASO) is the most common surgical procedure for the treatment of D-TGA. About 96% of children post ASO reaches adulthood. Breakthrough for surgical treatment of D-TGA occurred in the late 50s and early 60s with the introduction of the Senning and the Mustard procedure [1,2]. These operations were jointly termed “atrial switch procedures” which involved rerouting the systemic venous blood return from both caval veins through the left heart out the pulmonary artery. The pulmonary venous return is directed through the right heart out the aorta. However, the right ventricle has weaker valves and thinner walls designed to pump blood to the lungs, not systemically. Over time, the right ventricle cannot provide the necessary strength to pump blood systemically, leading to heart failure [3]. Currently, those born with D-TGA usually undergo arterial switch due to better long-term outcomes. The arterial switch was first performed by Jatene and his colleagues in 1975. This procedure encompasses switching the great vessels and re-implantation of the coronary arteries to the neo aorta. Obstruction of the coronary arteries may occur in 5-8% of patients, being the most common cause of mortality and morbidity post arterial switch operation [4].
Case Presentation
18-year-old male was referred for outpatient evaluation of exertional chest pain. He had history of D-TGA and underwent Rashkind Transcatheter Balloon atrial septostomy on the second day of life followed by arterial switch operation at one week of age. The Left Anterior Descending (LAD) coronary artery arose from sinus 1 and traveled intramurally. The right coronary artery and the left circumflex artery arose from sinus 2. During surgery, the right coronary artery and the left circumflex artery were excised separately, and the LAD artery was resected along with the surrounding tissue. Patient was followed by pediatric cardiologists until the age of 15 and course was uneventful. Upon initial patient care, his medical records were not available.
The chest pain was atypical in nature without any significant exertional dyspnea or syncope. He denied tobacco use but had been vaping for 4 years prior to presentation. On examination, vitals were stable. Auscultation of heart revealed a normal S1 and S2 without murmurs. The rest of the physical exam was within normal limits. Electrocardiogram showed sinus rhythm. Echocardiogram showed levocardia with normal ventricular systolic function and ejection fraction of 57%. Contrast computed tomography scan of the chest showed a 1.1x1.5x1.1 cm aneurysm of the proximal LAD artery (Figure 1). Findings were confirmed on Magnetic Resonance Imaging (Figure 2). Exercise myocardial perfusion imaging was also normal. The patient’s Adult Congenital Heart Disease Anatomical and Physiological classification was IIIA. Patient’s medical records were obtained and showed his LAD artery aneurysm diagnosis was madeaboutfiveyearsearlieratage13, and there was no interval progression since. After a multidisciplinary discussion, continued medical management was felt to be the best option for the patient with serial clinical follow-ups. On a 6-month follow-up, the patient continues to be doing well and has excellent functional capacity.
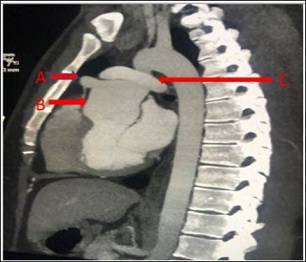
Figure 1: Cardiac CT A) Aneurysm of the proximal left anterior descending artery. B) Dilated aortic root. C) Pulmonary artery “draped” over the aorta post arterial switch surgery.

Figure 2: MRI showing A) Aneurysm of the proximal left anterior descending artery.B) Dilated aortic
Discussion
The number of adult patients who have undergone ASO in childhood is increasing. A patient who presents with chest pain post-ASO should be considered for morphological and functional assessment to exclude coronary artery disease. The process of the neoaortic root dilatation is known to be stable with minimal progression unless when associated with a ventricular septal defect, prior pulmonary artery banding, and in patients with Tausig Bing anomaly who develop severe progressive root enlargement. It is not known whether the proximal coronary artery aneurysm in the setting of ASO is also a stable process. This patient has had stable LAD aneurysm for the past five years. Currently no recommendation exists regarding management of LAD aneurysm in the setting of D-TGA following ASO. There is a need for a better understanding of the management of LAD aneurysm post ASO.
This patient’s presentation was unique since he also had an anomalous origin of the left circumflex artery originating from the sinus 2 together with the right coronary artery, and he had an intramural course of the LAD artery. Coronary anomaly is present in about 15-30% of patients with D-TGA. Intramural coronary course is associated with increased mortality and morbidity post ASO [5]. It is unclear whether the aneurysm of the LAD in our patient is due to the surrounding aortic tissue which was lifted together with the coronary artery.
Transfer and transition of care are important components of switching from pediatric to adult care in patients with congenital heart disease. Transfer indicates a point in time i.e. an event, whereby, the patient and the patient’s records are switched to the adult service from the pediatric service. Transition of care on the other hand is a gradual process of switching patient care. Transition involves a gradual increase of the responsibility of the patient’s health care and should be started early, usually around 12 years and be continued after transfer is made; usually by age 18 [6]. One of the most important transition models is the Congenital Heart Disease Transition Care model (CHDTC) which has been shown to improve knowledge, quality of life and health perception among adolescents during transition of care.
The attrition and lapse of care can both be prevented by early introduction of transition of care [7]. There are multiple reasons for lapse in care [8]. The major factor in our patient’s lapse in care was lack of insurance. Our patient was last seen in the pediatric cardiology clinic three years prior to his 18th birthday.
The guideline directed follow-up is once a year based on the Adult Congenital Heart Disease (ACHD) Anatomic and Physiologic (AP) classification of IIIA [6]. The prevalence of adult congenital heart disease is increasing and awareness of clinical presentation of these complex disease processes by general cardiology is essential. Equally important is coordination of care with the pediatric cardiologist in to facilitate safe transfer of care.
References
- Mustard WT (1964) Successful Two-stage correction of transposition of the great Surgery 55: 469-472.
- Senning A (1959) Surgical correction of transposition of the great Surgery 45: 966-980.
- Kiener A, Kelleman M, McCracken C, Kochilas L, St Louis JD, et (2018) Long-term survival after arterial versus atrial switch in d-transposition of the great arteries. Ann Thorac Surg 106: 1827- 1833.
- Angeli E, Formigari R, Pace Napoleone C, Oppido G, Ragni L, et (2010) Long-term coronary artery outcome after arterial switch operation for transposition of the great arteries. Eur J Cardiothorac Surg 38: 714-720.
- Metton O, Calvaruso D, Gaudin R, Mussa S, Raisky O, et (2010) Intramural coronary arteries and outcome of neonatal arterial switch operation. Eur J Cardiothorac Surg 37: 1246-1253.
- Stout KK, Daniels CJ, Aboulhosn JA, Bozkurt B, Broberg CS, et al. (2019) 2018 AHA/ACC guideline for the management of adults with congenital heart disease: Executive summary: A report of the american college of Cardiology/American heart association task force on clinical practice J Am Coll Cardiol 73: 1494-1563.
- Goossens E, Stephani I, Hilderson D, Gewillig M, Budts W, et al. (2011) Transfer of adolescents with congenital heart disease from pediatric cardiology to adult health care: An analysis of transfer des- J Am Coll Cardiol 57: 2368-2374.
- Yeung E, Kay J, Roosevelt GE, Brandon M, Yetman AT (2008) Lapse of care as a predictor for morbidity in adults with congenital heart Int J Cardiol 125: 62-65.
Citation: Mwansa V, Goyal A, Chandler JK, Talwar GS, Singh H, et al. (2020) 18 Years Old with History of D-TGA Post Arterial Switch Surgery Presented with Chest Pain Found to Have Left Anterior Descending Artery Aneurysm. J Cardio Cardiovasc Med 4: 018.
Copyright: © 2020 Mwansa V, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
